Authors: Meghan Christie, MD (EM Resident Physician, UPMC Emergency Medicine Residency), Aaron Brown, MD (Assistant Professor of Emergency Medicine, University of Pittsburgh School of Medicine; Curriculum Co-Director of Emergency Medicine Residency), and Kathy Gonzalez, MD (Surgery Resident Physician, UPMC Vascular Surgery Residency) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 62-year-old male with past medical history of hypertension and recent type B thoracic aortic dissection status post endovascular repair presents to the ED with complaints of upper back pain which started today. He describes the pain as constant, non-radiating, with no significant exacerbating or alleviating factors. On exam, he is hemodynamically stable with pulse 86, respiratory rate 14, blood pressure 138/90. Peripheral pulses are equal bilaterally, and neurologic exam is within normal limits.
Questions: How are aortic dissections managed surgically? What are the most common complications of both open surgical and endovascular repair of aortic dissection? How might these complications present? And, how are they managed?
Background
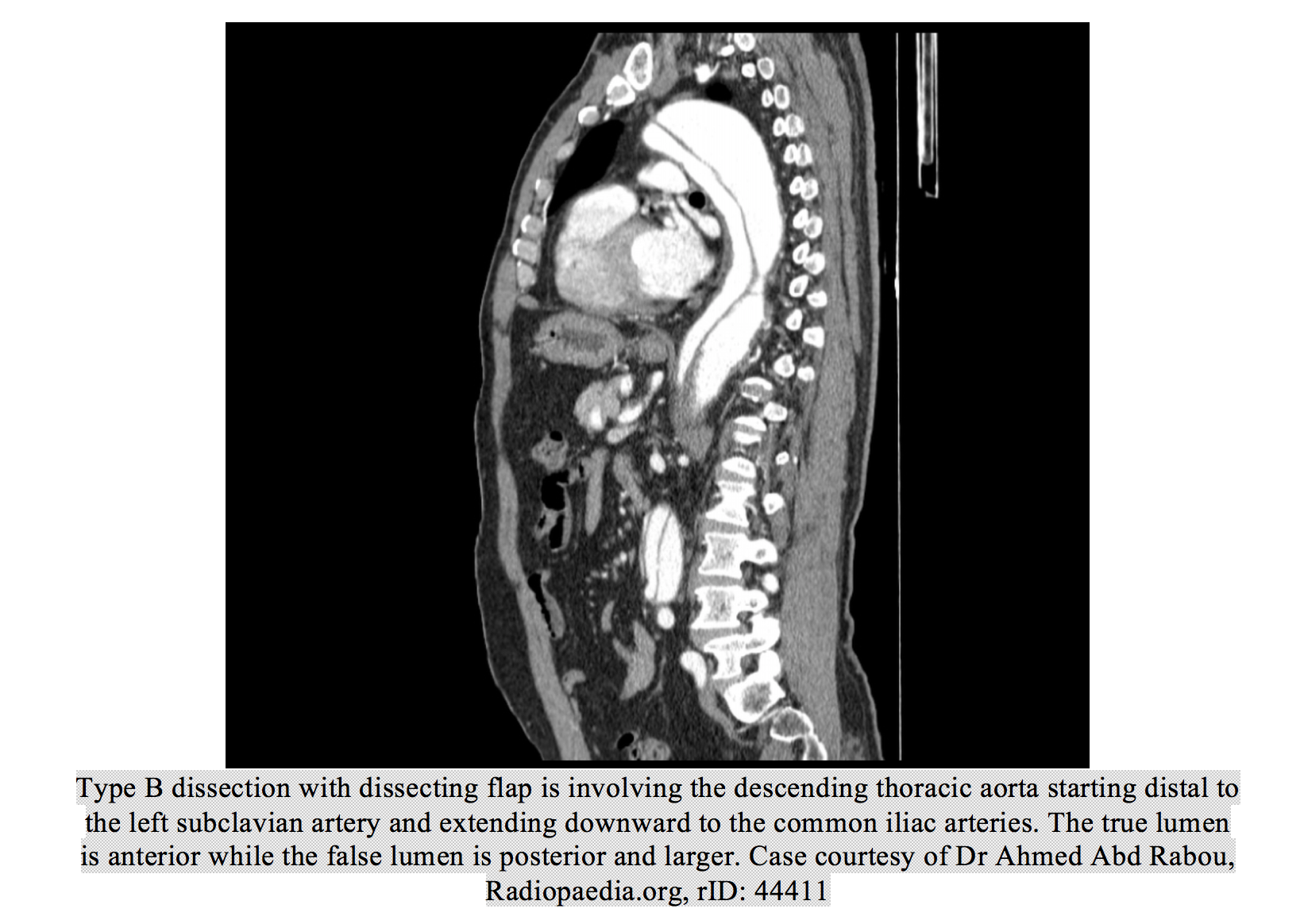
The incidence of aortic dissection is roughly 30 cases per million individuals per year.1 This includes both Stanford Type A dissections, which originate in the ascending aorta, as well as Type B dissections, which originate in the descending aorta, distal to the origin of the left subclavian artery. Type A dissection has a very high mortality, reportedly up to 1% per hour,1 as it is often complicated by aortic valve involvement, dissection into other great vessels, or dissection into the pericardium leading to tamponade. Type A dissection treatment often requires open surgical management, which may include coronary artery bypass graft (16% of cases), aortic valve repair or replacement (16% of cases), or aortic arch repair (19% of cases).2 Repair of Type A dissections may also include “arch debranching” which involves side-graft bypass to the brachiocephalic and left common carotid arteries to allow for graft replacement of more distal dissected thoracic aorta. Type B dissections have a lower mortality of about 10% at 30 days.1 Of Type B dissections, up to 70% tend to be uncomplicated,3 defined by dissection not involving distal ischemia, rupture, or rapidly expanding diameter. Uncomplicated Type B dissections have lower mortality and can often be managed medically with heart rate control, antihypertensives, and serial abdominal imaging for monitoring of disease progression. Though in the past complicated Type B dissections required open surgical repair, the mainstay of treatment has now become endovascular aortic repair (EVAR).

As mentioned, Type A dissections are managed almost exclusively with open surgical repair. Type B dissections, however, can be managed using either open surgical repair or endovascular repair. Management of descending aortic dissection is trending towards endovascular repair as the preferred treatment. In 2004, only 21% of Type B dissections were repaired endovascularly. This increased to 55% in 2007, which will likely continue to rise.4 This trend is supported by an evidence based improvement in morbidity and mortality with EVAR versus open surgery. One systematic review noted a reduction in all-cause 30 day mortality (OR 0.44, 95% CI [0.33-0.59]), and paraplegia (OR 0.42, 95% CI [0.28-0.63]), as well as decreased cardiac complications, reoperation for bleeding, renal dysfunction, pneumonia, and length of stay with thoracic endovascular aortic repair (TEVAR) versus open surgical repair of Type B dissections.5 A second study also showed reduced 30 day mortality (4.2% v 17.8%), shorter length of stay, less respiratory failure, and fewer wound complications with TEVAR when compared to open repair.4 Complications specific to open versus TEVAR as well as incidence and management are discussed below.
Complications and management
Complications following open surgical repair of Type A or B dissections
Stroke: Strokes occur at presentation in approximately 6-7% of patients with type A aortic dissection.2,6 The literature on postoperative strokes following open repair of dissection is sparse but is more likely in repair of Type A dissections involving arch replacement and to occur within the first few days postoperatively. Imaging of the aorta and neck vessels with CTA as well as head imaging should be used to ascertain vessel and graft patency in suspected postoperative stroke.
Aneurysmal Degeneration: Aneurysmal degeneration of the aorta distal to graft placement can occur and may involve the celiac, mesenteric, or renal arteries and compromise blood flow to these areas. One small study suggests that this complication can occur in up to 5% of patients following open aortic dissection repair.7 CT angiography of the aorta should be obtained if this is suspected, and management will often require open reoperation.
Graft Rupture: Aortic rupture at the graft site is a rare complication of open aortic repair. This may involve a contained rupture where bleeding is controlled by surrounding structures. Contained ruptures are typically managed by urgent reoperation. Uncontained ruptures are typically associated with severe hemodynamic instability and are often fatal.7
Complications following endovascular repair of Type B dissections
Postoperative complications following endovascular repair of Type B dissections include endoleak, distal true lumen collapse, retrograde dissection, paraplegia, stroke, stent-graft migration, lower limb ischemia, stent-graft fracture, and stent-graft infection with or without aorto-enteric fistula. Presentation, frequency, and possible treatment of these complications will be discussed below.8
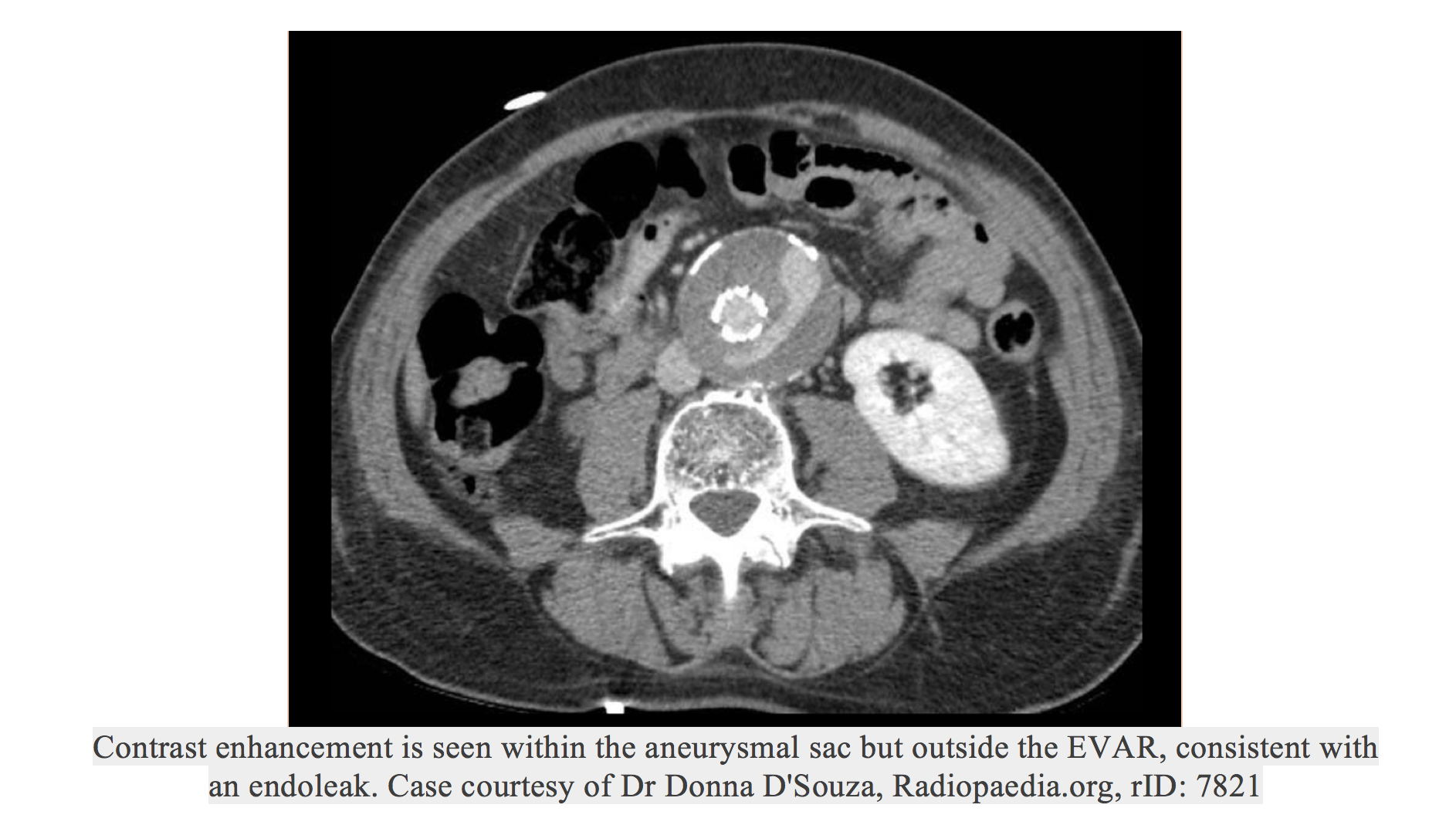
Endoleak: Most endoleaks are asymptomatic. However, if symptomatic, they may present with symptoms similar to an expanding abdominal aortic aneurysm, such as nonspecific back, flank, or abdominal pain. If ruptured, the patient will likely present with hemodynamic instability. There are four types of endoleaks. Type I is due to an incomplete seal at the graft attachment sites. Type II is due to the presence of patent mesenteric, lumbar, or intercostal branches. Type III is due to a junctional leak between graft components, and Type IV is a leak through the graft fabric. Imaging with CTA may show expansion of the false lumen outside of the stent-graft. One study shows approximately 28% endoleak complication rate in patients following a stent-graft for a Type B dissection.8 Definitive treatment may involve additional stent-grafts, ballooning of the original stent-graft, branch coil embolization, or conservative medical management.7
Distal lumen collapse: Collapse of the aortic lumen distal to the stent-graft may cause decreased blood flow distal to the graft leading to ischemia or claudication. In severe cases, this may result in increased pressure proximal to the stent-graft, with secondary rupture and hemothorax. An isolated study showed a 28% distal true lumen collapse complication rate in patients following a stent-graft for a Type B dissection.8 Definitive treatment may involve additional stent placement.
Retrograde dissection: Dissection in a retrograde direction, proximal to the stent-graft, may present with tearing chest pain or other dissection type symptoms. Imaging with CTA or transesophageal echocardiogram will show new flap development proximal to the stent-graft. Lui et al. reported a 10% retrograde dissection complication rate in patients following a stent-graft for a Type B dissection.8 Definitive treatment may involve surgical intervention or medical management.
Stroke: Strokes can occur by proximal pushing of the stent-graft leading to coverage of the left carotid artery, causing decreased cerebral blood flow.8 Strokes can also occur due to atheroma dislodgement of an atheroma by the wire during catheter-based interventions, though this mechanism is an acute peri-operative complication and would likely not be seen in the Emergency Department. Imaging of the aorta and neck vessels with CTA or MRA as well as head imaging will be required in this patient group. Studies show an 8-10% stroke complication rate in patients following a stent-graft for a Type B dissection.8 However, as many as 90% of these present in the acute postoperative period.2 Stroke following TEVAR has been shown to have a mortality of roughly 33%.2 It is important to consider this mechanism in patients with TEVAR history, as these are often managed with bypass surgery rather than thrombolytic medication or endovascular intervention.
Stent-Graft (SG) Migrations/Fractures: Stent-graft migrations may present with limb ischemia, paraplegia, or stroke like symptoms as the stent migrates and occludes other vessels. A 10% stent-graft migration complication rate has been reported in patients following a stent-graft for a Type B dissection.8 Definitive treatment may involve surgical intervention. Stent-graft fracture may present with acute chest pain sometimes years after stent placement. CT will show a fractured stent and expanded false lumen.8 The same study showed approximately a 3% stent-graft fracture complication rate in patients following a stent-graft for a Type B dissection.8 Definitive treatment may involve deployment of new stent-grafts to repair the fracture.
Lower limb ischemia: May present with pain, paresthesias, pallor, or decreased pulses in the lower extremities. Liu et al reported an 8% stent-graft extremity ischemia complication rate in patients following a stent-graft for a Type B dissection.8 Definitive treatment involves femoral bypass surgery or stent implant following balloon dilation.
Stent-Graft Infections and Fistulas: Endograft infection rate following any endovascular aortic surgery, not just dissection repair, has a reported incidence of 0.05-4%. Similar incidence is reported in open aortic surgery as well.9 This is usually an early complication, occurring at a median of 90 days,9 and most occurring within the first 6 months.10 This complication will usually require graft explantation via either an open or endovascular procedure.9 One study reported a 100% mortality in endograft infections treated with medical management alone.10 Patients will also typically receive antibiotic treatment for 4-6 weeks and life-long suppressive antibiotics.9 In most cases, infection is thought to be due to some other secondary source causing transient bacteremia and seeding of the endograft.9 Fistulas are also a relatively early complication of endovascular aortic repair occurring at a median of 3 months post-initial surgery.10 Fistulas are believed to be formed by close proximity of the graft to surrounding tissues. These tissues can become inflamed either at time of initial placement or secondary to graft infection, which can cause erosion and fistula formation.9 Fistula development typically requires emergent surgical management. Mortality of endovascular infection has been reported at 39% at 2 years, higher in those patients with fistula development (60%) and in those with thoracic stent infections (83%).9

ED Evaluation and Management: If the patient is unstable, clinicians should initiate appropriate resuscitative measures and consider bedside point of care ultrasound to assess for bleeding, dissection flap, aortic rupture, volume status, aortic flow, and tamponade. Emergent consultation with vascular/thoracic surgery for possible intervention should not be delayed. For stable patients, imaging of the aorta with CT angiography is likely the next appropriate step when possible. Transesophageal or transthoracic echocardiogram can be considered in situations where CTA is not possible to evaluate for proximal aortic complications. In the setting of stroke-like symptoms, an MRI/MRA may be appropriate for assessing stroke burden and vessel patency prior to planned interventions. A full physical exam including peripheral pulses and focused neurologic evaluation should be performed to evaluate for ischemia. It is important to know the type of dissection, whether Type A or Type B, as well as the type of repair the patient underwent, as potential complications can vary with each (described above). Transfusion should be based on patient appearance and hemodynamics.
Pearls
– Type A dissections almost always require open surgical repair, whereas Type B dissections can often be managed medically, if uncomplicated, or with endovascular repair. The type of repair predicts potential complications and should be considered when evaluating a post-operative dissection patient.
– TEVAR is now favored compared to open repair of Type B dissections as this has been shown to reduce morbidity and mortality.
– The most common post-operative complications following endovascular repair of type B dissections include endoleak, distal true lumen collapse, retrograde dissection, paraplegia, stroke, SG migration, lower limb ischemia, and SG fracture.
– Overall 30-day mortality after a SG placement is approximately 6.4%, higher in those undergoing emergent (vs. elective) treatment.
– In patients with recent EVAR, an ED physician should have a high index of suspicion for these complications in patients with back, flank, abdominal, or chest pain, as well as in those with vascular/neurologic compromise.
– ED management should include a focused neurovascular exam with head imaging as needed, CT angiography of the aorta, and vascular/thoracic surgery consultation.
References
- Criado, F. Aortic Dissection, A 250-year perspective. Texas Heart Institute Journal 2011; 38(6): 694-700.
- Hagan, PG, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. Jama 2000; 283(7): 897-903.
- Gutsche, J. T., et al. Risk factors for perioperative stroke after thoracic endovascular aortic repair. The Annals of Thoracic Surgery 2007; 84(4): 1195-1200.
- Chou, H, et al. Outcome comparison between thoracic endovascular and open repair for Type B aortic dissection: A population-based longitudinal study. Journal of the Chinese Medical Association 2015; 78:241-248.
- Cheng, D, et al. Endovascular Aortic Repair Versus Open Surgical Repair for Descending Thoracic Disease. Journal of the American College of Cardiology 2010; 55(10):986-1001.
- Chou, H, et al. Outcome comparison between thoracic endovascular and open repair for Type B aortic dissection: A population-based longitudinal study. Journal of the Chinese Medical Association 2015; 78:241-248.
- Hagan, PG, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. Jama 2000; 283(7): 897-903.
- Bavaria, J. E., Brinster, D. R., Gorman, R. C., Woo, Y. J., Gleason, T., & Pochettino, A. Advances in the treatment of acute type A dissection: an integrated approach. The Annals of thoracic surgery 2002; 74(5): S1848-S1852.
- Murphy E, et al. The management of endograft infections following endovascular thoracic and abdominal aneurysm repair. Journal of Vascular surgery 2013;58(5):1179-1185.
- Nozdrzykowski, M, et al. Outcomes of secondary procedures after primary thoracic endovascular aortic repair. Journal of Cardio-Thoracic Surgery 2016; 49: 770-777.
Further Reading
- Alsac, J, et al. The significance of endoleaks in thoracic endovascular aneurysm repair. Ann Vasc Surg 2011; 25:345-351.
- Ameli-Renani, S, Das, R, Morgan, R. Thoracic Endovascular Aortic Repair for the Treatment of Aortic Dissection: Post-operative Imaging, Complications, and Secondary Interventions. Cardiovasc Intervent Radiol 2015; 28:1391-1404.
- Qin, Y, et al. Endovascular Repair Compared with Medical Management of Patients with Uncomplicated Type B Acute Aortic Dissection. Journal of the American College of Cardiology 2016; 67(24) 2835-2842.
- Andersen, G, et al. Current management and outcomes of chronic type B dissection: results with open and endovascular repair since the advent of thoracic endografting. Ann Cardiothorac Surg 2014; 3(3): 264-274.
- Conway, A, et al. Outcomes of open surgical repair for chronic type B aortic dissections. Society for Vascular Surgery 2014; 59(5): 1217-1223.
- Lui, Z, et al. Treatment of serious complications following endovascular aortic repair for type B thoracic aortic dissection. Journal of International Medical Research 2017; 0(0)1-11.
- Piffaretti, G, et al. Complications after endovascular stent-grafting of thoracic aortic diseases. Journal of Cardiothoracic Surgery 2006; 1:26







