
Clinical Case: Bounceback Leg Pain
By Jessica Lopez MD
EM Resident Physician
NYU/Bellevue
Edited by Adaira Landry MD and Stephen Alerhand MD
Chief Complaint: Right Leg Pain
First Visit
History of Present Illness:
An 82 year-old female with newly diagnosed atrial flutter 7 days prior to presentation (taking Coumadin and Enoxaparin bridge therapy) presents to the ED stating after noticing right leg pain for the past couple of days. The pain was more severe this morning, worsened upon lying down and better with movement. She denies shortness of breath, chest pain, or abdominal pain. She also denies numbness, loss of sensation, tingling, muscle weakness, or loss of motion in the right leg. Patient is able to bear weight and denies trauma. Of note, the patient’s Hb was 14 on last admission.
Medical Hx: as above
Medications: as above
Allergies: NKDA
Surgical Hx: denies
Social Hx: +social EtOH
Physical Exam:
Vitals: BP 146/94, HR 72 bpm, RR 14, 100% RA, Temp 97.9, Pain 8/10
Gen: NAD, well-appearing
Cardiopulmonary: wnl
Musculoskeletal: Minimal swelling noted to the right leg, no tenderness noted upon palpation of calf or leg, full ROM of leg noted
Neurological: AAOx3
Labs:
BMP 134/4.2, 98/25, 29/0.8, glucose 150, calcium 8.6, PT39/PTT53/INR 3.8, CBC 10> Hb 11 /34<185
Imaging:
Right Lower Extremity Venous Duplex: Negative for deep venous thrombosis
XR Right femur: No acute fracture or dislocation; mild degenerative hip changes
ED Course: The patient’s pain decreased to 2/10 while in the ED and she was able to ambulate. INR was 3.8, thus enoxaparin held. Patient given strict precautions for which to return, along with outpatient follow up instructions.
Discharge diagnosis: Muscular pain
Outpatient visit the following day
The patient reported back pain and was sent for outpatient MRI to rule out lumbar disc disease. The MRI showed possible right psoas bleed, and the patient was sent back to the ED.
Bounceback Visit
Patient returned to the ED complaining of back pain and persistent right leg pain. A CT of the abdomen/pelvis demonstrated a retroperitoneal hematoma. Patient’s INR was now 5 and hemoglobin had fallen to 8.5. The patient was given Vitamin K 10 mg IV, 1500 Units 4-factor PCC (Kcentra), and 2U PRBC. She was admitted to the MICU. The patient was evaluated by the General Surgery consult, who recommended checking CBC q4h without acute surgical intervention. The patient remained stable throughout the hospital stay and was discharged after two days on a lower dose of Coumadin.
Background Information
Retroperitoneal hematoma is a rare but serious complication of anticoagulation, and may also be seen in hemophiliacs. The retroperitoneal space confers danger in a bleeding patient, as it may go unrecognized and be missed on many point-of-care diagnostic interventions (i.e. ultrasound).
Key Bedside Signs:
The physical exam is very important in diagnosis of a patient with retroperitoneal hematoma.
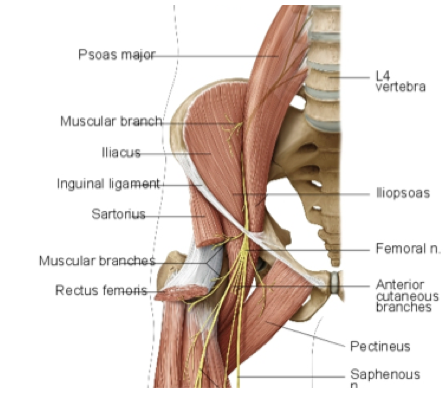
- Retroperitoneal hematomas may cause a femoral nerve neuropathy. The femoral nerve is composed of nerve roots L2-L4, which coalesce under the psoas muscle in the pelvis. When a retroperitoneal hematoma becomes clinically significant, the nerve roots are compressed as they travel under the psoas muscle and down through the inguinal canal. This can produce the sensation of numbness over the anteromedial thigh, quadriceps weakness, and decreased or absent patellar reflex (mediated by L4).
Figure I
- Occasionally, the patient may have a tender mass palpated in the abdomen, although this is rare.
- Ecchymosis is occasionally seen tracking under the inguinal ligament to the lower abdomen and groin. However, it is not usually seen until 2-3 days after hematoma development, and it requires that the blood tracks under the inguinal ligament.
Figure 2. Figure 3.
Figure 4. Figure 5.
- The psoas muscle will also be irritated by the accumulated blood, causing the patient to feel pain when the psoas is stretched (positive psoas sign) and alleviated when the knee/hip are flexed. The patient may also experience pain in the groin and lower back.
Imaging:
When suspected, the diagnostic modality of choice for retroperitoneal hematoma is CT scan with IV contrast. While there is some institutional variation, CT’s for retroperitoneal bleeds should view from just above the diaphragm to the greater trochanters. This patient underwent an outpatient MRI out of suspicion for lumbar disc disease. MRI should be able to identify a bleed, though it is not as sensitive as CT scan (current gold standard). Ultrasound is not a useful diagnostic modality in this scenario.
Management:
Generally, there are three ways to manage a retroperitoneal hematoma. Smaller hematomas may be managed non-operatively, if the patient is hemodynamically stable and otherwise well-appearing. With a clinically significant bleed, hemodynamic instability, or significant femoral neuropathy, surgical decompression may be considered. Surgical consult should be initiated for any significant bleed. Otherwise, interventional radiology may be involved in lumbar artery embolization, especially when there is active bleeding on CT scan (indicated by a blush, or leakage of contrast).
Errors in Case Management
- Lack of complete physical exam – Neither an abdominal exam nor a neurological exam of the lower extremities was documented for the initial encounter. It is unclear if the patient was fully undressed (ecchymosis possibly not recognized).
- The patient was seen by a junior level provider during a busy overnight shift. Was there appropriate oversight?
- The chart does not reflect that the providers addressed the hemoglobin drop in the first ED visit.
- Retroperitoneal hematoma is a rare diagnosis that may go unrecognized if not considered in the differential. Atraumatic muscular pain should be a diagnosis of exclusion in an 82 year-old female.
Take-away Points
- Maintain extremely high index of suspicion of bleed in any anti-coagulated patient or hemophiliac.
- Most bleeds occur within the first 3 months of coumadin initiation.
- While the incidence of bleed increases proportionally with the INR, most bleeds occur with therapeutic (2-3) INR. One should not be reassured by a “therapeutic INR.”
- Fully undress the patient and perform thorough skin exam.
- Perform a neurologic exam on patient with unexplained, seemingly muscular complaints.
- Pay close attention to patients on anticoagulation with a Hb drop, while suspecting a bleed. Even if the bleed is not identified, consider observing or even admitting the patient until a definitive diagnosis is made.
- When ordering tests, it is important to trend values and interpret them in the context of the clinical situation.
References
- Iliopsoas haematoma: a rare complication of warfarin Ozkan OF, Guner A, Cekic AB, Turan T, Kaya U, Reis E. J Coll Physicians Surg Pak. 2012 Oct;22(10):673-4.
- Iliopsoas muscle hematoma during treatment with warfarin. Zago G, Appel-da-Silva MC, Danzmann LC. Arq Bras Cardiol. 2010 Jan;94(1):e1-3.
- Acute groin pain and femoral nerve deficit in a warfarin treated patient. Thorgersen EB, Øfsti AM, Nyheim T, Abedini S. Tidsskr Nor Laegeforen. 2002 Oct 10;122(24):2360-1.
- Femoral neuropathy and retroperitoneal hemorrhage. Mastroianni PP, Roberts MP. Neurosurgery. 1983 Jul;13(1):44-7.
- Compressive femoral neuropathy: a rare complication of anticoagulation. Ong HS. Singapore Med J. 2007 Mar;48(3):e94-5.
- Figure 1 Taken from http://www.studyblue.com/notes/note/n/anatomy-for-bfcp2-practical–final/deck/4419713
- Figure 2 taken from http://www.studyblue.com/notes/note/n/hematologylymph-set-2/deck/1050296
- Figure 3 taken from http://www.studyblue.com/notes/note/n/ch-17-abdomen/deck/6953961
- Figure 4 taken from http://en.wikipedia.org/wiki/Cullen’s_sign
- Figure 5 taken from http://surgicomania.blogspot.com/2010/05/acute-pancreatitis-and-ca-pancreas.html





