Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Written by Lauren Hart, MD and Edited by Tim Greene, MD
Definition: Fracture of the calcaneus bone
Mechanism
- Traumatic axial loading is the most common cause (eg fall from height)
- Can also occur in MVCs when the accelerator/brake pedal impacts the foot
- Stress fractures seen with overuse from repetitive impact (e.g. runners)
Epidemiology
- 2% of all fractures
- Most frequently fractured tarsal bone
- 90% occur in men between 21 and 45 years of age with majority being industrial workers
- Approximately 10% are open fractures (Egol 2010)
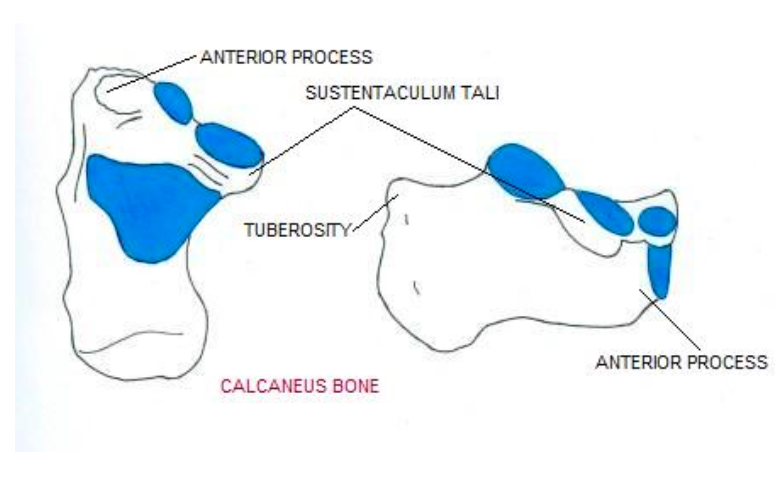
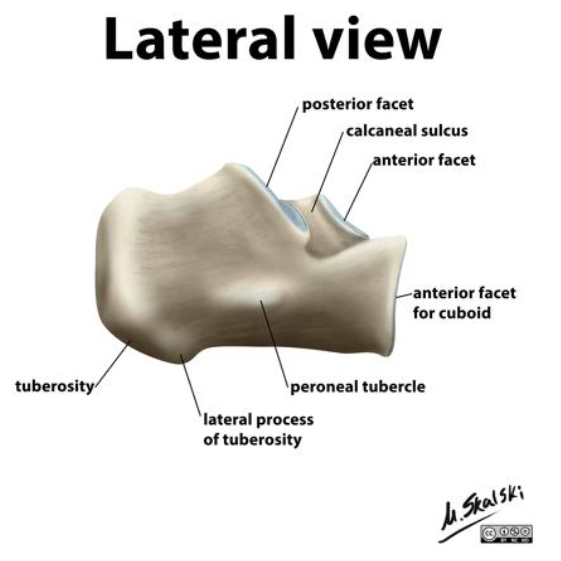
The Calcaneus (joint-pain-expert.net/calcaneus)

Ecchymosis after Calcaneus Fracture (orthopaedicsone.com)
Physical Exam
- Moderate to severe heel tenderness
- Swelling
- Shortened wide heel with varus deformity
- Ecchymosis around heel extending to arch is highly suggestive, may also see fracture blisters
- Compartment syndrome occurs in 10% of calcaneal fractures and can result in clawing of the toes after recovery (Egol 2010)
- Concomitant Achilles tendon rupture may be present
Calcaneus Fracture Classification (See Images in Gallery Below)
- Extra-articular (subtalar joint)
- 25% of all calcaneus fractures
- Avulsion injury of:
- Anterior process by bifurcate ligament
- Sustenaculum tali
- Calcaneal tuberosity (Achilles tendon avulsion)
 Intra-articular
Intra-articular
- 75% of calcaneus fractures
- 2 classification systems
- Essex-Lopresti Classification
- The primary fracture line runs obliquely through the posterior facet forming two fragments.
- The secondary fracture line runs in one of two planes:
- “Tongue-Type” Fracture
- Axial plane beneath the posterior facet exiting posteriorly
- This fracture tends to cause tension on the skin with possible necrosis. Consider an emergent orthopedics consult for all patients with this pattern (Snoap 2017)
- Behind the posterior facet in joint depression fractures
- “Tongue-Type” Fracture
- Sanders (based on CT)- based on number and location of articular fragments seen on the coronal CT image at the widest point of the posterior facet (E)
- Type I: all nondisplaced fractures
- Type II: two-part fractures of the posterior facet
- Type II: three-part fractures with centrally-depressed fragment
- Type IV: four-part articular fractures
- Essex-Lopresti Classification
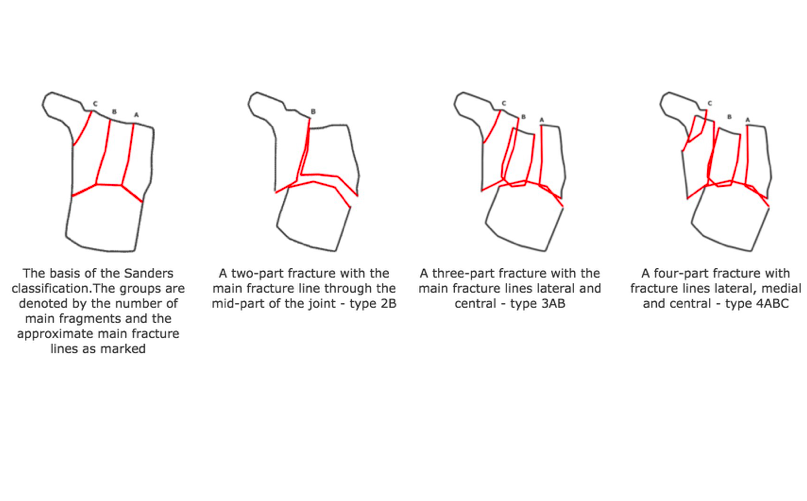
Sanders Classification (foothyperbook.com)
Calcaneus Fracture Classification Images

Anterior Process Fracture (orthobullets.com)

Achilles Avulsion (southfloridasportsmedicine.com)
Sustenaculum Tali Fracture (Gitjan 2014)
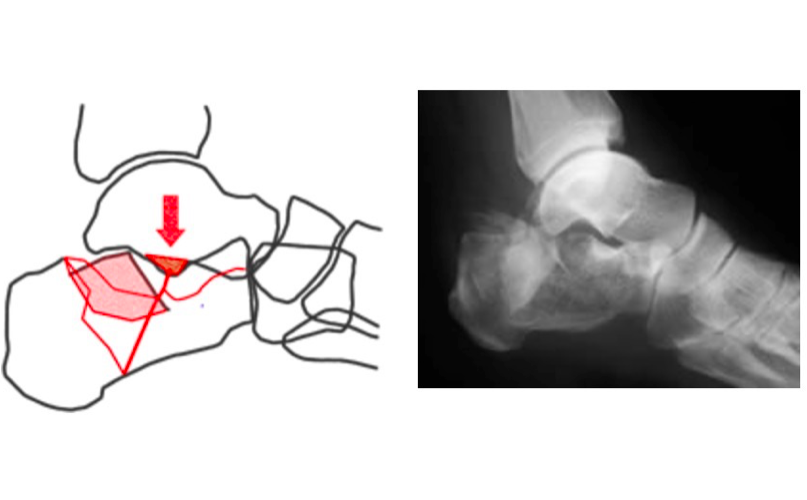
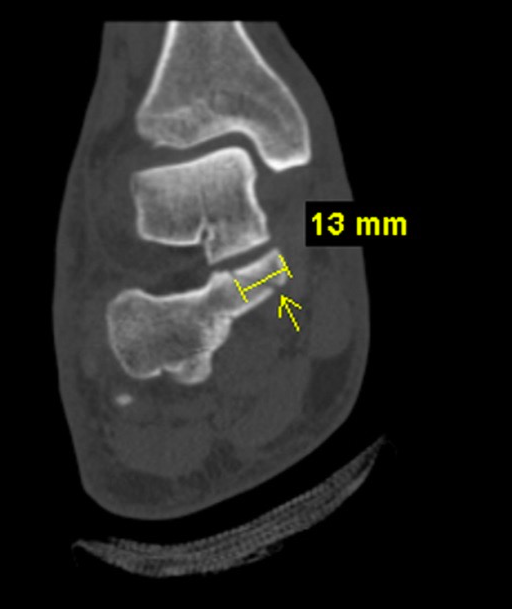
Joint Depression (foothyperbook.com)
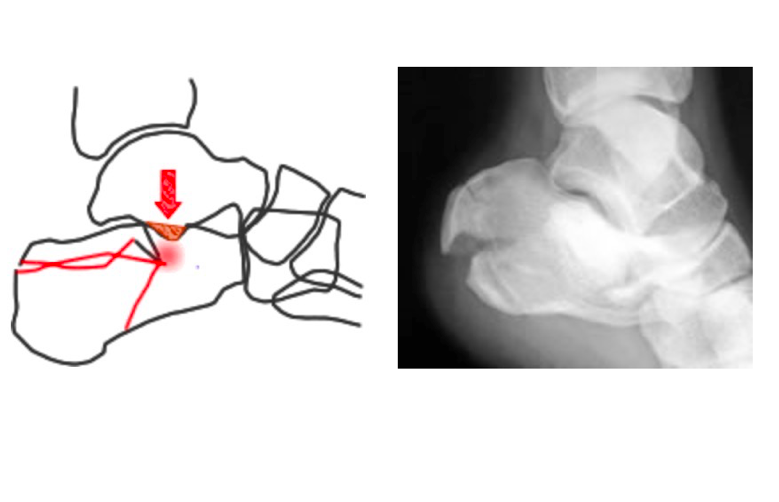
Tongue Type Fracture (foothyperbook.com)

Bohler Angle (orthobullets.com)
Diagnostic Imaging
- Standard X-rays: AP, lateral, oblique foot
- Optional X-rays (See Image Gallery below)
- Broden views: allows visualization of posterior facet
- Harris View: visualizes tuberosity fragment widening, shortening, and varus positioning
- AP ankle: demonstrates fibular impingement if lateral wall extrusion is present
- Findings in calcaneal fractures:
- Reduced Bohler angle
- Created with lines drawn tangiental to anterior and posterior aspects of superior calcaneus
- Normal is 20-40 degrees
- Increased angle of Gissane
- Formed by downward and upward slopes of calcaneus
- Normal is 95-105 degrees
- Non-contrast CT
- Obtain when clinical suspicion of a fracture is high despite negative x-rays
- Gold standard imaging test for any calcaneal fracture (except for stress fractures)
- Will almost always be obtained for pre-operative planning but does not necessarily need to be obtained in the ED

Angle of Gissane (orthobullets.com)
Associated Injuries
- Vertebral injuries secondary to axial loading injury (10%)
- Contralateral calcaneal injury (10%) (Hatch)
Optional X-ray Images
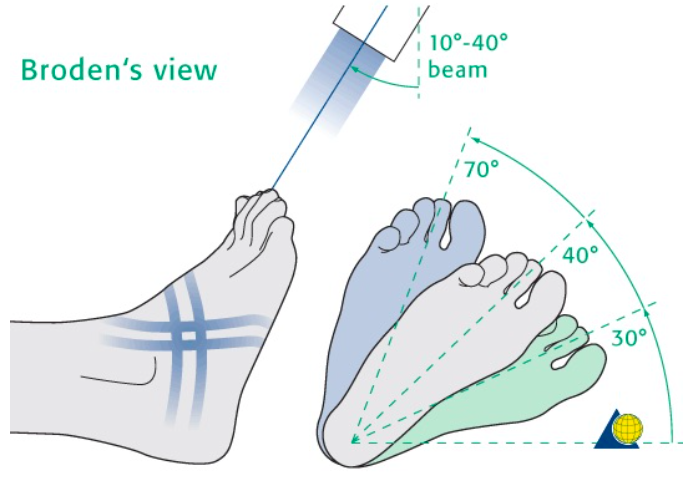
Broden’s View (myradiographer.com)
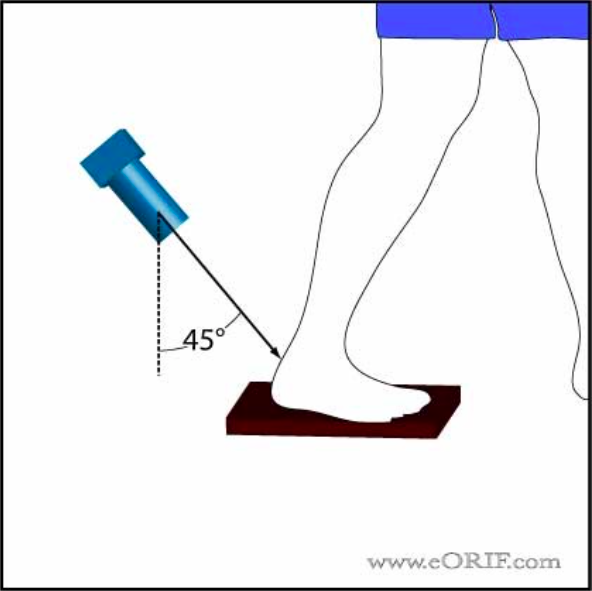
Harris View (eorif.com)
ED Management
- Provide analgesia
- Complete neurovascular exam
- Consider compartment syndrome
- Can initially be placed in Bulky Jones dressing with supportive posterior splint to provide flexion
- Conservative therapy (casting + nonweightbearing)
- Casting and nonweightbearing for 6 weeks for calcaneal stress fractures
- Casting and nonweightbearing for 10-12 weeks if:
- Small extra-articular fracture (<1 cm) with intact Achilles tendon and <2 mm displacement
- Sanders Type I (nondisplaced)
- Anterior process fracture involving <25% of calcaneocuboid joint
- Comorbidities that preclude good surgical outcome (smoker, diabetes, PVD)
- All other fractures require surgical intervention
Prognosis: Relatively poor with overall 40% complication rate (malunion, subtalar arthritis, clawing of toes)
Take Home Points
- Always suspect calcaneus fractures in patients with axial loading injuries to the lower extremities. If a calcaneus injury is found, look for concomitant fractures of the ankle and vertebrae.
- Patients with calcaneal fractures will always be nonweightbearing on ED discharge
- Watch out for compartment syndrome of the foot which occurs in 10% of calcaneal fractures and results in significant morbidity
Read More
Ortho Bullets: Calcaneus Fractures
References
- Barrie J. (2013) Calcaneal fractures. [East Lancashire Foot and Ankle Hyperbook]. Link
- Egol KA et al. Handbook of Fractures 4th ed. Lipincott 2010: 507-519.
- Gitajn IL et al. Anatomic alignment and integrity of the sustenaculum tali in intra-articular calcaneal fractures. J Bone Joint Surg Am. 2014; 96(12): 1000-1005. PMID: 24951735.
- Snoap T et al. Calcaneal Fractures: A Possible Musculoskeletal Emergency. J Emerg Med 2017.52 (1), 28-33 PMID: 27658550






