
Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Written by: Anand Swaminathan, MD
Definition:
A serum calcium level < 8.5 mg/dL or an ionized calcium level < 2.0 mEq/L
Background
- Exists in two states
- Free ionized form (approx. 50%)
- Bound to other molecules (primarily albumin)
- Ionized Ca2+ concentration is inversely proportional to pH
- Ca2+ metabolism
- Vitamin D: aids in intestinal Ca2+ absorption
- Parathyroid hormone (PTH)
- Increases renal Ca2+ reabsorption
- Arbitrates Vit D stimulated intestinal Ca2+ absorption
- Mobilizes Ca2+ from bone
- Calcitonin
- PTH antagonist
- Inhibits renal Ca2+ reabsorption
- Inhibits Ca2+ mobilization from bone
- Ca2+ plays numerous critical roles including muscle contraction (skeletal and smooth), clotting factor activity and nerve conduction
Causes
- Hypoalbuminemia (Ca2+ bound to albumin)
- Hypoparathyroidism
- Chronic renal failure
- Electrolyte disorders: Hypomagnesemia, Hyperphosphatemia
- Abnormal cell destruction: tumor lysis syndrome, rhabdomyolysis
- Severe pancreatitis
- Drugs: Calcitonin, phosphate, bisphosphonates
- Tox: HFl acid burn
- Massive blood transfusion (due to citrate in blood products)
Clinical Manifestations
- Cardiac Effects
- Hypotension
- QTc prolongation
- Congestive heart failure
- Cardiovascular collapse (severe hypocalcemia)
- Neuromuscular Effects
- Muscle cramping
- Paraesthesias
- Tetany
- Chvostek’s sign: facial muscle twitching with tapping over facial nerve (commonly seen in patients without hypocalcemia)
- Trousseau’s sign: carpal spasms induced by inflation of a blood pressure cuff 20 mm Hg above systolic BP X 3 minutes
- Other symptoms
- Altered mental status
- Coarse hair
- Cataracts
- Poor dentition
- Dry skin
- Laryngospasm
- Bronchospasm, wheezing
- Fatigue
Hypocalcemia EKGs
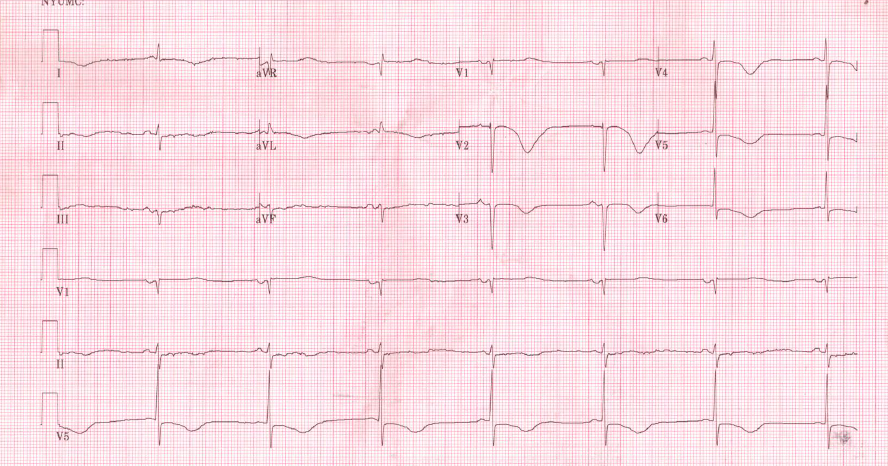
QTc Prolongation Ca 2+ = 7.4
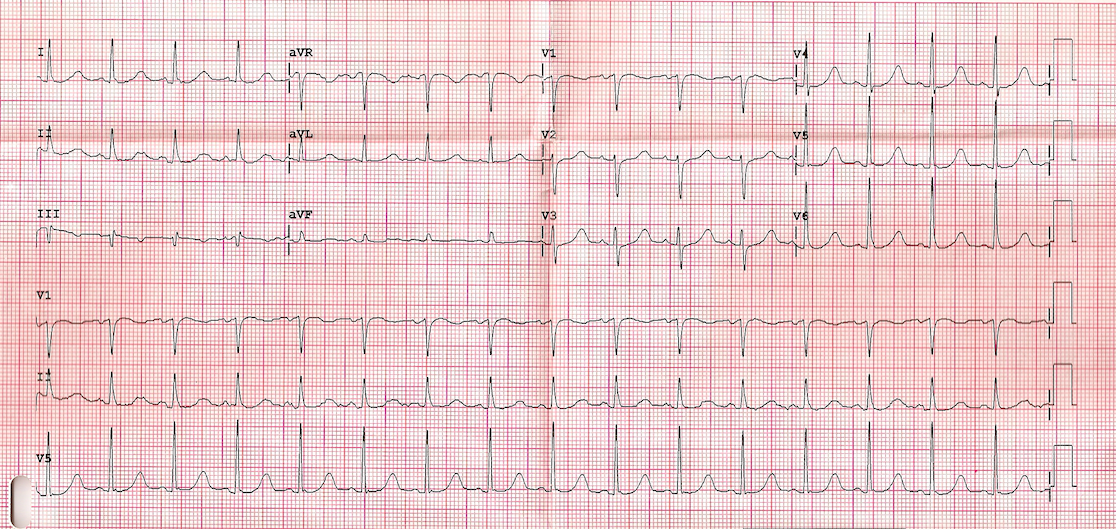
QTc Prolongation Ca 2+ = 7.9
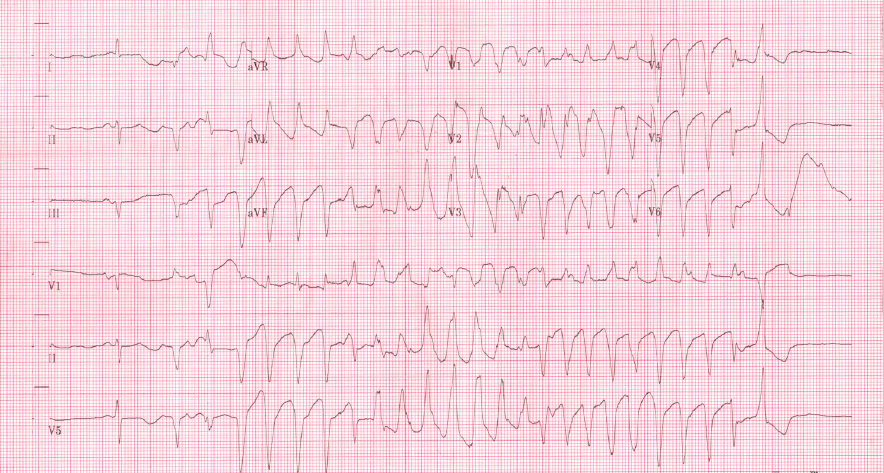
Torasdes de Pointes in Hypocalcemia
Diagnosis
- Serum calcium < 8.5 mg/dL
- Correct for hypoalbuminemia:1 g/dL drop in serum albumin below 4 g/dL = 0.8 mg/dL drop in serum calcium
- 50% of serum calcium is protein bound, 50% ionized (free)
- Ionized calcium < 2.0 mEq/L
- More accurate assessment as no correction required
Management
- Asymptomatic/Minimally symptomatic
- Oral supplementation with calcium salts (i.e. calcium carbonate or calcium citrate)
- Disposition: Discharge home with outpatient follow up
- Moderate/Severe Symptoms
- Intravenous calcium supplementation: 100-300 mg Ca2+ raises serum Ca2+ by 0.5 – 1.5 mEq
- Calcium Chloride (CaCl2)
- Standard “ampule”: 10 ml of 10% CaCl2 = 270 mg of Ca2+
- Caustic to veins – should be administered in large peripheral IV or central line preferably
- Calcium Gluconate
- Standard “ampule”: 10 ml of 10% CaGluconate = 90 mg of Ca2+
- For equivalent dosing to CaCl, give 3 “amps” of CaGluconate
- Despite classic teaching, CaCl2 is not more bioavailable than CaGluconate and does not raise serum Ca2+ faster. (Hayes 2013)
- Disposition: Admission to monitored setting if ongoing intravenous repletion (bradycardia and hypertension may occur)
- Consider giving prophylactic calcium supplementation in patients receiving massive transfusions.
- Magnesium supplementation: Concomitant hypomagnesemia is common.
Take Home Points
- Severe hypocalcemia can cause hypotension and QTc prolongation leading to Torsades de Pointes.
- Treat moderate to severe symptoms and any EKG changes with IV calcium salts
- Always search for and treat the underlying cause of hypocalcemia
References:
Pfenning CL, Slovis CM: Electrolyte Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 125: p 1636-53.
Hayes BD. (2013, July 2). Mythbuster: Calcium Gluconate Raises Serum Calcium as Quickly as Calcium Chloride [ALiEM]. Retrieved from http://www.aliem.com/posts/
Read More
LITFL: Hypocalcemia
LITFL: Hypocalcaemia






2 thoughts on “CORE EM: Hypocalcemia”
Pingback: CORE EM: Hypocalcemia – Global Intensive Care
Pingback: Episode 30: Hypocalcemia Resulting from Trauma & Blood Product Transfusion - The Pharm So Hard Podcast