Author: Lloyd Tannenbaum, MD (Emergency Medicine Resident, San Antonio, TX) // Edited by: Jamie Santistevan, MD (@jamie_rae_EMdoc – EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD (@MPrizzleER – Assistant Professor of Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center); and Brit Long, MD (@long_brit – EM Attending Physician, San Antonio, TX)
Welcome to ECG Pointers, an emDOCs series designed to give you high yield tips about ECGs to keep your interpretation skills sharp. For a deeper dive on ECGs, we will include links to other great ECG FOAMed!
This week we are continuing our Syncope Series with a discussion of Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). Interestingly, much like Hypertrophic Cardiomyopathy (HCM), this disease process has another name, Arrhythmogenic Right Ventricular Dysplasia, but currently, ARVC is the preferred term for this disease state. As a quick refresher, any patient that presents with syncope should have a thorough history and physical performed and an ECG. These recommendations are based off of the ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope which has been endorsed by ACEP as guidelines for clinical practice [1]. As previously discussed, screen every ECG for DQ@HEB [2]:
D: Delta wave (Wolff-Parkinson-White)
Q: QT Prolongation
@: AV nodal blocks
H: HCM (look for dagger Q waves)
E: Epsilon wave (Arrhymogenic Right Ventricular Dysplasia/Cardiomyopathy)
B: Brugada
The Case:
A 22-year-old military trainee presents unconscious in ventricular tachycardia. His battle buddies tell you that he was running a fitness test and suddenly passed out. After several rounds of CPR and multiple shocks, you achieve ROSC. The post-ROSC ECG is shown below:
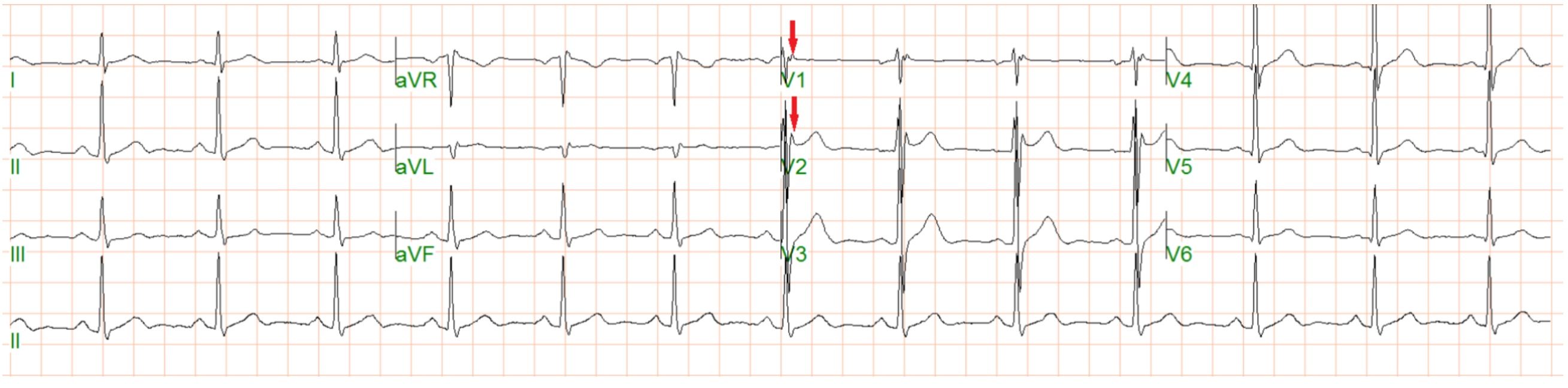
This ECG shows normal sinus rhythm with a rate of approximately 80 bpm. Of note, there appears to be an extra wave at the end of the QRS complexes seen best in V1 marked with a red arrow. ECG compliments of Dr. James Kimber [3].
Why did this previously healthy trainee go into VT? Could this have been predicted? What is going on with his ECG?
To figure out what is going on, we need to start with a discussion of the extra wave seen in this ECG. This extra wave is known as an epsilon wave and was first described by Dr. Guy Fontaine in 1977. An epsilon wave is most often associated with Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). In this disease process, the right ventricular myocardium is replaced by fibro-fatty tissue. It is present in up to 20% of patients who experience sudden cardiac death. Wondering why the name “epsilon wave” was chosen? Well, first let’s look at when the wave occurs. Looking back at the ECG above, we see that the epsilon wave occurs after the QRS complex. This makes sense because the myocardium is filled with fat, and fat conducts electricity slower than the natural conduction pathway of the heart. The electricity showing up on an ECG after the QRS complex makes it a Post-Excitation wave. When Dr. Fontaine was coming up with a name for this wave, he chose epsilon because a delta wave was used for pre-excitation, and as epsilon follows delta in the greek alphabet, epsilon should be used for post-excitation [4]
ECG changes noted in ARVC are varied, and interestingly, progressive. In 1996, Dr. Jaoude published a paper that looked at the changes over time in patient’s ECGs with AVRC. What he found is depicted below from his paper:

Note that the most common finding in ARVC is not an epsilon wave, but rather T wave inversions in lead V1-3. This is however a nonspecific finding on an EKG, whereas the epsilon wave is much more specific for ARVC. There are many different changes to an EKG that can occur as a result of ARVC such as T wave inversions in V1-V3 and epsilon waves, as mentioned earlier, but also left or right bundle branch block, widening of the QRS complexes, and a prolonged S wave upstroke. Also note that ARVC is a progressive disease, with all patients having an abnormal ECG 6 years after initial episode of ventricular tachycardia and subsequent diagnosis of ARVC [5].
2-D Echo or Cardiac MRI can be used to help make the diagnosis. See below for a cardiac MRI of a patient with ARVC:

This image shows fatty infiltration of both the left and right ventricle [6].
The history of Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC) is a little difficult to track down. Dr. Osler noted in the sixth edition of his text, “The Principles and Practice of Medicine (1905)” the existence of a condition where the walls of the heart would become “thin as parchment,” but in this case, he was describing the entire heart, not just a specific ventricle [7]. Then, in 1952, Dr. Henry Uhl published a paper on a rare condition he named, “Uhl’s Anomaly.” Patients with this disease get dyspnea, syncope on exertion, and arrhythmias. While this is similar to ARVC, they do not get the fibro-fatty replacement of the myocardium, rather they have a congenital absence of the myocardium of the right ventricle [8]. In 1977, one of the earliest cases of ARVC was described by Dr. Fontaine and his colleagues, [9] but it took until 1982 for the clinical signs and symptoms of this condition to be described [10]. The study to do this was a case study of 24 patients diagnosed with ARVC was published by Drs. Marcus and Fontaine. What they found was that patients can presents in Ventricular Tachycardia, Supraventricular Arrhythmias, Right Heart failure, or Asymptomatic Cardiomegaly [9]. Also, in the 24 patients, 16 of them were male, leading to the classic teaching of a 3:1 male to female prevalence [9]. Dr. Marcus’s paper was also the first to note a genetic component to the disease, when he found multiple members of the same family with ARVC [10]. It is now known that the disease follows an autosomal dominant inheritance pattern. Classically, the disease has been described as more prevalent in people of Greek or Italian descent, but families with 2 or more members with ARVC have been recognized all over the world [11]. Worldwide, the prevalence of this disease is 1:5000 [11]. That takes us to the present day. In 1994, a task force assembled to come up with diagnostic criteria for ARVC, which was later revised in 2010.
Diagnosing ARVC is a complicated task best left to the cardiologists. For the 2010 diagnostic criteria, see this report from an International Task Force designed to diagnose ARVC:
https://www.ahajournals.org/doi/pdf/10.1161/CIRCULATIONAHA.108.840827
Case Conclusions: The patient was taken to the MICU and eventually made a full recovery. He had a cardiac MRI showing right ventricular akinesis and an epsilon wave on his EVG, consistent with ARVC.
References/Further Reading:
- Shen W-K, Sheldon RS, Benditt DG, Cohen MI, Forman DE, Goldberger ZD, Grubb BP, Hamdan MH, Krahn AD, Link MS, Olshansky B, Raj SR, Sandhu RK, Sorajja D, Sun BC, Yancy CW, 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope, Journal of the American College of Cardiology (2017), doi: 10.1016/j.jacc.2017.03.003.
- Kann, Kristen. Professional Mneumonicer.
- Kimber J R, Sabzwari S, Ayele H (June 07, 2018) Syncopal Episodes of Arrhythmogenic Right Ventricular Cardiomyopathy in a Patient with Pre-existing Seizure Disorder. Cureus 10(6): e2760. DOI 10.7759/cureus.2760
- Hurst, JW. Naming of the Waves in the ECG, With a Brief Account of Their Genesis. Circulation. 3 Nov 1998.98:1937-42.
- Jaoude, SA, Lrclercq, JF, Coumel, P. Progressive ECG changes in Arrhythmogenic Right Ventricular Disease. European Heart Journal. 1996. 17: 1717-22.
- Segal HN: Parchment heart(Osler). Am Heart J 40:948,1950.
- Te Riele, Anneline SJM, et al. “Noninvasive multimodality imaging in ARVD/C.” JACC: Cardiovascular Imaging 8.5 (2015): 597-611.
- Vecht RJ, Carmichael DJ, Gopal R, et alUhl’s anomaly.Heart 1979;41:676-682.
- Fontaine G, Guiraudon G, Frank R, Vedel J, Grosgogeat Y, Cabrol C, Facquet J. Stimulation studies and epicardial mapping in ventricular tachycardia: study of mechanism and selection for surgery. In: HE Kulbertus (ed). Reentrant Arrythmias. Lancaster, Pa: MTP Publishing; 1977; 334–350.
- Marcus FI, Fontaine GH, Guiraudon G, Frank R, Laurenceau JL, Malergue C, Grosgogeat Y. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384–398.







