
Authors: Zain Javaid, MD (EM Resident Physician, Zucker-Northwell NSLIJ); Marianne Haughey, MD (@mthaughey, EM Attending Physician, Zucker-Northwell LIJ) // Reviewed by: Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY) and Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 36-year-old female presents to the ED with vaginal pain. She initially noticed a small bump one week ago that was only painful with sexual intercourse, but it has grown and now causes discomfort even when walking. Her temperature is 98.9oF, heart rate 78, and blood pressure 126/84. On exam she has a large, soft mass protruding at the 8 o’clock position of the vaginal opening that is painful and fluctuant to touch. There is some induration around the mass, but no vaginal discharge is noted on the pelvic exam.
What is most likely causing this woman’s pain? How would you manage this diagnosis to provide some relief?
Answer: Bartholin’s Abscess
Background:
- Bartholin’s glands[1]
- Pea-sized glands located bilaterally at the 4 o’clock and 8 o’clock positions of the posterior introitus
- Provide lubrication to the vagina by secreting mucus via ducts into the introitus
- If normal, usually cannot be felt by simple palpation

Epidemiology:
- 2% of women have a lifetime incidence of a Bartholin’s cyst or abscess[3]
- Much more common in reproductive-age women
Pathogenesis:
- When a Bartholin’s duct is obstructed, mucoid secretions cannot be released[3,4]
- Secretions build up inside the duct and eventually form a Bartholin’s cyst[4]
- If the cyst becomes infected, it develops into a Bartholin’s abscess
- However, an abscess does not always need a cyst to precede it
- Initially thought to be caused solely by STI organisms, but that is no longer the case[3]
History:
- Important points to consider[4,5]
-
- How long have symptoms been occurring?
- What is the extent of the patient’s pain? Is it occurring with simple movements such as walking or intercourse?
- History of prior Bartholin’s cyst or abscess?
- Obtain a thorough sexual history to differentiate various genital lesions
Physical Exam:[3,5]
- Perform both an external and internal exam to determine extent of patient’s symptoms
- Important points to consider during your exam:
-
- Are there multiple lesions?
- Is the lesion painful?
- Are there any overlying skin changes?
- Are there systemic symptoms?
- If there is vaginal discharge or cervical motion tenderness, an STI etiology may be more likely
Clinical Presentation:[5]
- Usually painful, unilateral, and located at the 4 o’clock or 8 o’clock position
- A Bartholin’s cyst, while located in the same position, is usually not painful
- Fluctuant mass with possible induration/erythema on overlying skin
- May already be draining purulent fluid
Differential Diagnosis:
- Soft Lesion: Bartholin’s cyst, Bartholin’s abscess, Skene’s duct cyst, Epidermal inclusion cyst[3,5]
- Firm Lesion: Leiomyoma, Lipoma, Squamous cell carcinoma[3,5]
Management:
- Rarely resolves on its own. If a patient has pain, intervention will likely be needed[6]
- Treatment begins with an incision and drainage. Afterwards, a Word catheter or Jacobi ring must be used
- I&D: This step will be like any other I&D
- Anesthetize the area with lidocaine
- Using a #11 blade, make a vertical incision posterior to the labia minora. This location will prevent notable scarring
- Break up loculations with a hemostat to allow proper drainage
- Send off a culture after collecting purulent fluid on a culture swab
- However, a Bartholin’s abscess I&D is not a definitive treatment[7]
- ~13% of patients will have recurrent abscess
- This is due to premature closure of the tract which prevents further drainage
- To allow continued drainage and thereby prevent recurrence, a Word catheter or Jacobi ring should be placed
- Word catheter: Short, rubber catheter with a balloon tip[8]

- Word catheter provides a tract for continued drainage of the abscess[10]
- Pus does not flow out through the catheter itself. It drains from the space between the mucosa and rubber catheter
- Steps to place a Word catheter[11,12]
- Once the incision is made and fluid is drained, place the catheter through the opening
- After the catheter is placed, inflate the balloon with saline. This will prevent it from being dislodged when the patient goes home
- The Word catheter stays in place for 2-4 weeks until it is removed
- For removal: Balloon is deflated, and the catheter is simply pulled from the abscess cavity

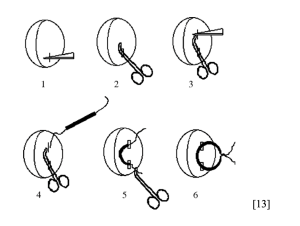
- To place a Jacobi ring:[13]
- Inject lidocaine
- Make an initial stab into the mucosa
- Break up loculations with a hemostat
- Create a tract with the hemostat and make another stab incision into the other end of the tract
- Take tubing from a butterfly catheter (cut off the needle end) and pass it through the tract you created
- Tie the two ends of the tubing, but be sure not to tie too tightly
- Antibiotics[11]
- Should only be given if a patient has a recurrent Bartholin’s abscess or if there is overlying cellulitis
- Should cover Gram-positive organisms, including MRSA
- Choices include Bactrim 800mg/160mg BID x7 days or Doxycycline 100mg BID x7 days
- Consider IV antibiotics for immunocompromised patients or those with poorly controlled diabetes
- For further care at home, the patient should do Sitz baths and refrain from intercourse[8]
- Patient should follow up with an OB/GYN after discharge due to risk of recurrence
Take Home Points:
- If a patient presents with a painful fluctuant mass near the introitus and you suspect a Bartholin’s abscess, intervention is almost always needed
- A simple I&D is usually not a definitive treatment for a Bartholin’s abscess
- A Word catheter or Jacobi ring can prevent recurrence of a Bartholin’s abscess
- Antibiotics are needed for recurrent abscesses, overlying cellulitis, or an immunocompromised patient








2 thoughts on “EM@3AM: Bartholin’s Abscess”
Pingback: ≫ emDOCs.net – Educación en medicina de emergenciaEM@3AM: Absceso de Bartholin - emDOCs.net
Pingback: Quiz 171, December 9, 2022 – The FOAMed Quiz