Authors: Russ Burgin (MS4, Bethesda, MD); Rachel Bridwell, MD (EM Attending Physician, WA) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 34-year-old male is brought via EMS after collapsing during an outdoor adventure race. EMS reports the patient was conscious but altered, with slurred speech and confusion. Point of care glucose in the field was 102 mg/dL.
Triage vital signs include BP 80/40 mm Hg, HR 154 bpm, T 41C rectal, RR 28 breaths per minute, saturation 94% on room air. The patient is agitated, not oriented, and becoming combative with ED staff. A 12-lead EKG shows sinus tachycardia but is otherwise normal. As you attempt to examine the patient, he has a generalized, tonic-clonic seizure.
What is your diagnosis, and what are your next steps in evaluation and management?
Answer: Hyperthermia1-22
Background:
- Definition: body temperature greater than the body’s regulatory set point1
- Pathophysiology: excessive external heat load, metabolic heat production, ineffective heat dissipation, hypothalamic dysfunction, or combination overwhelm heat regulation mechanisms1,8
- Fever occurs when the hypothalamus elevates the body’s temperature set point in response to infection or inflammation.1
- Fever is usually < 40C.
- Temps greater than 41.5C are highly suggestive of hyperthermia2
- In hyperthermia, the body has lost control of thermal regulation
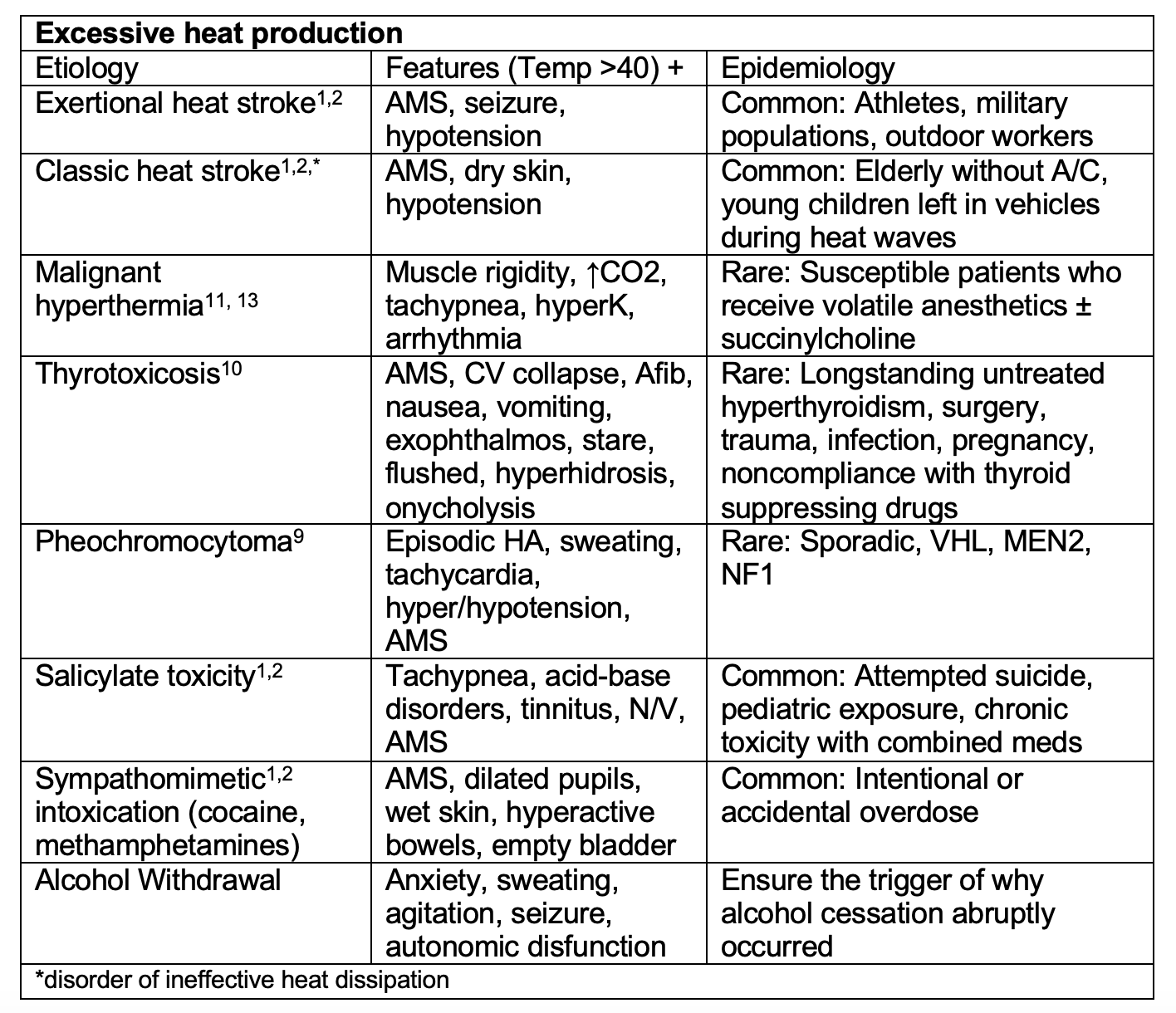
Etiologies:

Evaluation:1,8
- Identify/treat underlying cause – medication/ingestion/exercise history
- ABCDEs/Vital signs
- Continuous core temp monitoring18,19
- Bladder probe for non-intubated patients
- Esophageal probe for intubated patients
- Rectal probes may lag in measurement
- Look for toxidromes – examine pupils, auscultate bowel sounds, sweat (wet in sympathomimetic vs dry in anticholinergic)
- ECG: arrhythmias
- CBC, Coags: DIC
- CMP/UA: electrolyte derangements (hypoglycemia, hyponatremia), AKI, liver failure
- TSH: thyroid storm
- APAP/salicylate level/UDS: overdose
- CK: rhabdomyolysis
- CXR: ARDS
- Neuroimaging (CT/MRI): if concern for brainstem stroke or other neurological cause
Treatment:
- Address underlying cause if not pure heat stroke
- Obtain IV/IO access, fluid resuscitation
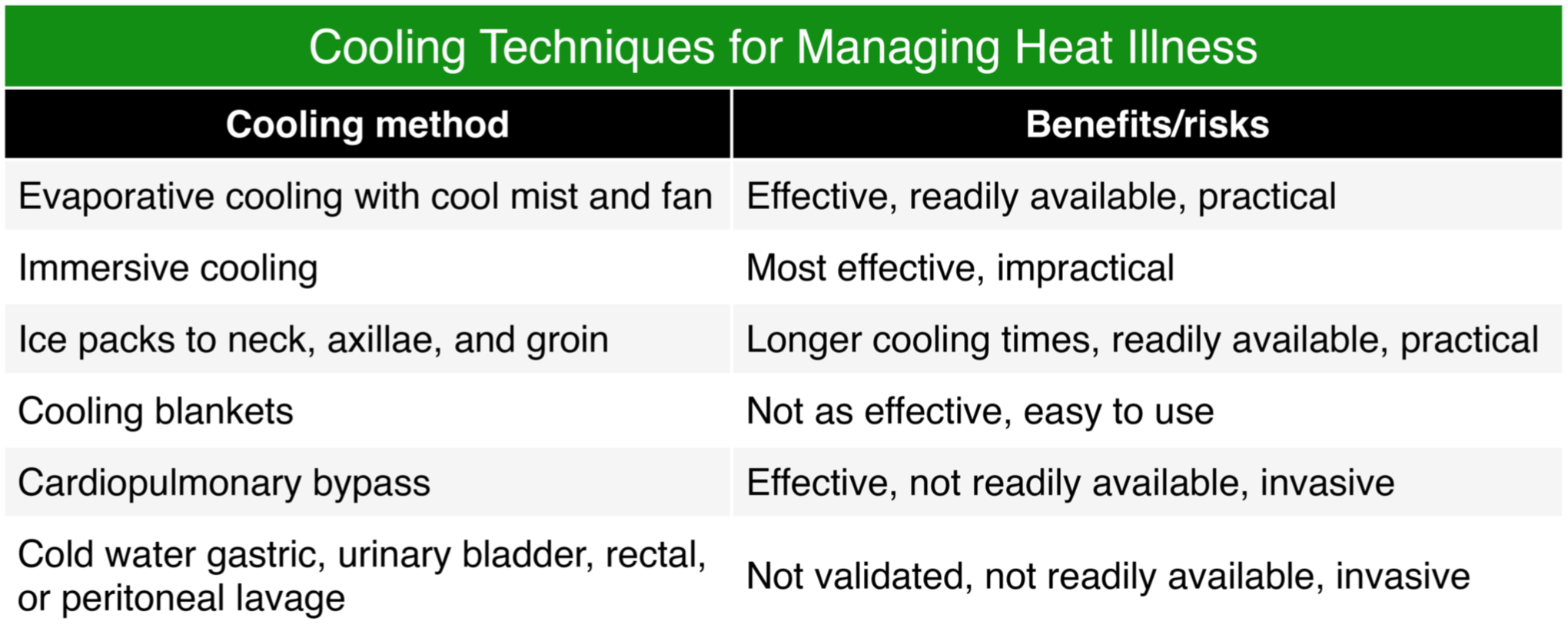
- Resuscitative Cooling
- Gold standard = Ice water immersion (DT 0.2C per minute)1,4
- Body bag may be utilized if no immersion tank available3
- Evaporative cooling (DT 0.1C per minute)1
- Spray naked patient with lukewarm/tepid water
- Direct fans over body
- Can be combined with ice packs in axilla/groin/neck
- Will not work in relative humidity > 70%
- Gold standard = Ice water immersion (DT 0.2C per minute)1,4
- Benzodiazepines26
- Seizure treatment or if concern for toxicology source/agitation
- Lorazepam 4 mg IV push over 2 minutes (may be repeated in 5-10 min if seizure activity continues)
- Diazepam 10 mg IV or rectal (may be repeated as above)
- Midazolam 10 mg IV (may also be given IM if no IV access
- Lorazepam 1-2 mg IV or midazolam 2.5-5mg IM or IV for agitation alone
- Benzos may help improve core cooling27
- No known role for antipyretics aside from known treatable causes
- Adjuncts
- Cooled IV fluids 4C (DT 2C per 2L)
- 1L per 30 minutes
- If the patient needs volume, give cold volume
- Dehumidified high flow nasal canula14 or disconnect humidifier from ventilator circuit (may also use nasal cannula on intubated patient)15
- Uses surface area of turbinates/lungs to dissipate heat
- ECMO as last resort or if indicated for another problem
- Thoracic, peritoneal or bladder lavage17
- Cooled IV fluids 4C (DT 2C per 2L)
- Endpoint: Target <40C in first 30-60 minutes with endpoint of 38-39C to avoid overshooting to hypothermia16
- Consider intubation:16
- Airway protection
- Paralysis for decreased heat production from muscular contraction/agitation
- Prophylactically for extending imaging studies or transport
- Consider repeat boluses before pressors
- Peripheral vasoconstriction may trap heat
Complications:
- CNS – AMS, coma, seizures, cerebral edema, cerebellar ataxia21
- Cardiac: tachyarrhythmias, acute decompensated heart failure, ST changes, prolonged QT, transient Brugada pattern20
- Respiratory – aspiration, ARDS, bronchospasm, pulmonary edema23
- Metabolic derangements – respiratory alkalosis, metabolic acidosis, hypo/hyperkalemia, hyponatremia, hypoglycemia, hypocalcemia1
- Hematologic derangements – DIC, thrombocytosis, leukocytosis
- AKI/Renal Failure1
- Hepatic Failure – normally self-limited, but may require transplantation22
- Rhabdomyolysis – muscle injury, dehydration, AKI
- Compartment syndrome8
Pearls:
- Hyperthermia is inappropriately elevated temperature, usually greater than 40C.
- Determine and treat underlying cause, consider multiple etiologies.
- Rapid cooling is the primary treatment. When cooling is achieved within 30 minutes, mortality approaches zero percent.28
- Continuous core temp monitoring via esophageal or bladder probe until stable at < 39C.
- Cold water immersion is the gold standard if you are equipped for it; otherwise use evaporative cooling and always consider adjunctive measures.
- Assess for and treat known complications (DIC, electrolyte derangements, etc.).

An 18-month-old boy presents to the emergency department with loss of consciousness. He was found unresponsive alone in a hot vehicle. His initial vital signs show a temperature of 43.1°C, heart rate of 210 bpm, respiratory rate of 50/minute, and blood pressure of 82/34 mm Hg. An IV is placed and basic labs are obtained. His blood glucose is 152 mg/dL, pH is 7.12, carbon dioxide is 32 mEq/L, and lactate is 7.1 mmol/L. He is intubated and a bolus started. Which of the following is the best next step to treat this patient?
A) Broad-spectrum antibiotics
B) Chilled intravenous normal saline
C) Cold water immersion
D) Evaporative cooling
Answer: D
Classic heat-related illness is most seen in young children unable to escape from hot environments. Exertional heat illness is most seen in adolescents who engage in heavy exercise during periods of high temperature and humidity (e.g., football players, military). Both can result in heat exhaustion and heat stroke and have many overlapping symptoms. Patients with heat exhaustion typically have dizziness, tachycardia, headache, nausea, vomiting, and profuse sweating. Patients with heat stroke have hot, dry skin and altered mental status (e.g., convulsions, delirium). By definition, heat exhaustion occurs with a core temperature of 37.7–39.4°C, and heat stroke occurs at a core temperature > 40°C. This applies only to heat-related illness, not patients with a fever. The development of central nervous system dysfunction may be as subtle as impaired judgment or inappropriate behavior, and the progression to loss of consciousness may be abrupt. When heat stroke is severe, unconsciousness may persist even after the temperature is lowered.
Treatment is by lowering the body temperature as rapidly as possible. Evaporative cooling is the preferred method to actively reduce body temperature in the emergency department, as it can be performed with ongoing resuscitation efforts. This is performed by undressing the patient, spraying or sponging tap water onto the patient, and using multiple fans to blow air across the patient’s skin. Ice packs can also be placed at the neck, groin, and axilla. Ice water immersion and iced peritoneal lavage are additional methods used to lower temperature but are more invasive or can prevent additional resuscitative efforts. Methods to actively cool patients should be stopped when the temperature drops to below 38.5°C. Sedation and paralysis are helpful to prevent shivering during cooling attempts. Heat stroke can lead to end-organ dysfunction such as rhabdomyolysis, disseminated intravascular coagulation, cardiogenic shock, liver failure, and cerebral edema.
Broad-spectrum antibiotics (A) for septic shock are not inappropriate given the hyperthermia, tachycardia, and hypotension. However, without signs of infection and with a history of being left in a hot car, antibiotics are less likely to benefit this patient than active cooling.
Chilled intravenous normal saline (B) results in cardiac dysrhythmia and should not be used to treat heat stroke.
The most effective way to actively reduce temperature is cold water immersion (C), but most patients will need intubation, sedation, and paralysis, and this interferes with monitoring and additional treatment.
Further Reading
Additional FOAM Resources:
- https://emcrit.org/ibcc/hyperthermia/#(1)_internal_cooling:_crystalloid
- https://litfl.com/hyperthermia-associated-toxidromes/
- https://litfl.com/hyperthermia/
References:
- Epstein, & Yanovich, R. (2019). Heatstroke. The New England Journal of Medicine., 380(25), 2449–2459. https://doi.org/10.1056/NEJMra1810762
- Simon. (1993). Hyperthermia. The New England Journal of Medicine, 329(7), 483–487. https://doi.org/10.1056/NEJM199308123290708
- Kim, D. A., Lindquist, B. D., Shen, S. H., Wagner, A. M., & Lipman, G. S. (2020). A body bag can save your life: a novel method of cold water immersion for heat stroke treatment. Journal of the American College of Emergency Physicians open, 1(1), 49–52. https://doi.org/10.1002/emp2.12007
- Douma, Aves, T., Allan, K. S., Bendall, J. C., Berry, D. C., Chang, W.-T., Epstein, J., Hood, N., Singletary, E. M., Zideman, D., & Lin, S. (2020). First aid cooling techniques for heat stroke and exertional hyperthermia: A systematic review and meta-analysis. Resuscitation., 148, 173–190. https://doi.org/10.1016/j.resuscitation.2020.01.007
- Gaudio, & Grissom, C. K. (2016). Cooling Methods in Heat Stroke. The Journal of Emergency Medicine., 50(4), 607–616. https://doi.org/10.1016/j.jemermed.2015.09.014
- Bouchama, Dehbi, M., & Chaves-Carballo, E. (2007). Cooling and hemodynamic management in heatstroke: practical recommendations. Critical Care : the Official Journal of the Critical Care Forum., 11(3). https://doi.org/10.1186/cc5910
- Broessner G, Beer R, Franz G, Lackner P, Engelhardt K, Brenneis C, Pfausler B, Schmutzhard E. Case report: severe heat stroke with multiple organ dysfunction – a novel intravascular treatment approach. Crit Care. 2005 Oct 5;9(5):R498-501. doi: 10.1186/cc3771. PMID: 16285034; PMCID: PMC1297610.
- Asplund, O’Connor, F. G., & Noakes, T. D. (2011). Exercise-associated collapse: an evidence-based review and primer for clinicians. British Journal of Sports Medicine., 45(14), 1157–1162. https://doi.org/10.1136/bjsports-2011-090378
- Kakoki, K., Miyata, Y., Shida, Y., Hakariya, T., Takehara, K., Izumida, S., Sekino, M., Kinoshita, N., Igawa, T., Fukuoka, J., & Sakai, H. (2015). Pheochromocytoma multisystem crisis treated with emergency surgery: a case report and literature review. BMC research notes, 8, 758. https://doi.org/10.1186/s13104-015-1738-z
- Swee, duS., Chng, C. L., & Lim, A. (2015). Clinical characteristics and outcome of thyroid storm: a case series and review of neuropsychiatric derangements in thyrotoxicosis. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists, 21(2), 182–189. https://doi.org/10.4158/EP14023.OR
- Larach, M. G., Gronert, G. A., Allen, G. C., Brandom, B. W., & Lehman, E. B. (2010). Clinical presentation, treatment, and complications of malignant hyperthermia in North America from 1987 to 2006. Anesthesia and analgesia, 110(2), 498–507. https://doi.org/10.1213/ANE.0b013e3181c6b9b2
- Velamoor V. R. (1998). Neuroleptic malignant syndrome. Recognition, prevention and management. Drug safety, 19(1), 73–82. https://doi.org/10.2165/00002018-199819010-00006
- Boyer, E. W., & Shannon, M. (2005). The serotonin syndrome. The New England journal of medicine, 352(11), 1112–1120. https://doi.org/10.1056/NEJMra041867
- Chava, R., Zviman, M., Raghavan, M. S., Halperin, H., Maqbool, F., Geocadin, R., Quinones-Hinojosa, A., Kolandaivelu, A., Rosen, B. A., & Tandri, H. (2017). Rapid Induction of Therapeutic Hypothermia Using Transnasal High Flow Dry Air. Therapeutic hypothermia and temperature management, 7(1), 50–56. https://doi.org/10.1089/ther.2016.0016
- Chava, R., Zviman, M., Assis, F. R., Raghavan, M. S., Halperin, H., Maqbool, F., Geocadin, R., Quinones-Hinojosa, A., Kolandaivelu, A., Rosen, B. A., & Tandri, H. (2019). Effect of high flow transnasal dry air on core body temperature in intubated human subjects. Resuscitation, 134, 49–54. https://doi.org/10.1016/j.resuscitation.2018.10.020
- Lipman, G. S., Gaudio, F. G., Eifling, K. P., Ellis, M. A., Otten, E. M., & Grissom, C. K. (2019). Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Heat Illness: 2019 Update. Wilderness & environmental medicine, 30(4S), S33–S46. https://doi.org/10.1016/j.wem.2018.10.004
- Horowitz B. Z. (1989). The golden hour in heat stroke: use of iced peritoneal lavage. The American journal of emergency medicine, 7(6), 616–619. https://doi.org/10.1016/0735-6757(89)90285-4
- Casa, D. J., Becker, S. M., Ganio, M. S., Brown, C. M., Yeargin, S. W., Roti, M. W., Siegler, J., Blowers, J. A., Glaviano, N. R., Huggins, R. A., Armstrong, L. E., & Maresh, C. M. (2007). Validity of devices that assess body temperature during outdoor exercise in the heat. Journal of athletic training, 42(3), 333–342.
- Moran, D. S., & Mendal, L. (2002). Core temperature measurement: methods and current insights. Sports medicine (Auckland, N.Z.), 32(14), 879–885. https://doi.org/10.2165/00007256-200232140-00001
- Lacunza, San Román, I., Moreno, S., García-Molina, E., Gimeno, J., & Valdés, M. (2009). Heat stroke, an unusual trigger of Brugada electrocardiogram. The American Journal of Emergency Medicine., 27(5), 634.e1–634.e3. https://doi.org/10.1016/j.ajem.2008.09.036
- Yang, M., Li, Z., Zhao, Y., Zhou, F., Zhang, Y., Gao, J., … & Kang, H. (2017). Outcome and risk factors associated with extent of central nervous system injury due to exertional heat stroke. Medicine, 96(44).
- Martínez-Insfran, L. A., Alconchel, F., Ramírez, P., Cascales-Campos, P. A., Carbonell, G., Barona, L., Pons, J. A., Sánchez-Bueno, F., Robles-Campos, R., & Parrilla, P. (2019). Liver Transplantation for Fulminant Hepatic Failure Due to Heat Stroke: A Case Report. Transplantation proceedings, 51(1), 87–89. https://doi.org/10.1016/j.transproceed.2018.03.137
- Varghese, G. M., John, G., Thomas, K., Abraham, O. C., & Mathai, D. (2005). Predictors of multi-organ dysfunction in heatstroke. Emergency medicine journal : EMJ, 22(3), 185–187. https://doi.org/10.1136/emj.2003.009365
- Jang, S. H., & Seo, Y. S. (2021). Neurogenic fever due to injury of the hypothalamus in a stroke patient: Case report. Medicine, 100(13), e24053. https://doi.org/10.1097/MD.0000000000024053
- Sánchez-Manso JC, Gujarathi R, Varacallo M. Autonomic Dysfunction. [Updated 2022 Oct 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430888/
- Teran F, Harper-Kirksey K, Jagoda A. Clinical decision making in seizures and status epilepticus. Emerg Med Pract. 2015 Jan;17(1):1-24
- Hostler D, Northington WE, Callaway CW. High-dose diazepam facilitates core cooling during cold saline infusion in healthy volunteers. Appl Physiol Nutr Metab 2009; 34:582
- Casa DJ, Armstrong LE, Kenny GP, O’Connor FG, Huggins RA. Exertional heat stroke: new concepts regarding cause and care. Curr Sports Med Rep. 2012;11(3):115–123.






