
Author: Rachel Bridwell, MD (@rebridwell, EM Resident Physician, San Antonio, TX) // Edited by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 12-year-old male is brought to the ED by his mom for right eye swelling and pain. The patient reports it hurts when he looks around the room. He denies any headache, fever, weakness, neck stiffness, recent trauma, dental work, or travel. Review of systems is remarkable for a recent sinus infection. Vital signs are normal.
Pertinent physical examination findings: Right eye – erythematous and edematous upper and lower eye lid. Extraocular movements intact though painful, noted OD aPD, proptosis of OD. VA: OD 20/100, OS 20/20. Fundoscopic exam is not possible due to swelling. The mouth, ears, nose, face, and neck are otherwise normal.
What’s the next step in your evaluation and treatment?
Answer: Orbital cellulitis1-15
Epidemiology:
- Caused by sinus infection extension, traumatic inoculation, hematogenous spread
- Risk Factors: sinus infection, dental work, foreign bodies
- 10x more common in children, peak age 12 years1,2
- In children, infection more commonly originates in the sinuses (maxillary>ethmoid>frontal>sphenoid), with 38% of patients with multiple sinuses involved3,4
- In adults, infection commonly originates in frontal sinus; only 11% of patients have involvement of multiple sinuses
- Foreign body: wood carries a large bacterial load with poor outcomes, though no predominant organism5
- Causative bacteria: Upper respiratory flora, both aerobic and anaerobic
- S. pneumonia, H. influenza, M. catarrhalis, S. aureus, S. pyogenes, Bacterioides spp., Fusobacterium spp.
- Developed countries: S. aureus, Streptococcus spp. most common2
- In diabetic and immunocompromised patients: consider mucormycosis and aspergillosis (high mortality rate)6
- Adults have narrowed sinus ostia, generating, with more anaerobic infections2
- S. pneumonia, H. influenza, M. catarrhalis, S. aureus, S. pyogenes, Bacterioides spp., Fusobacterium spp.
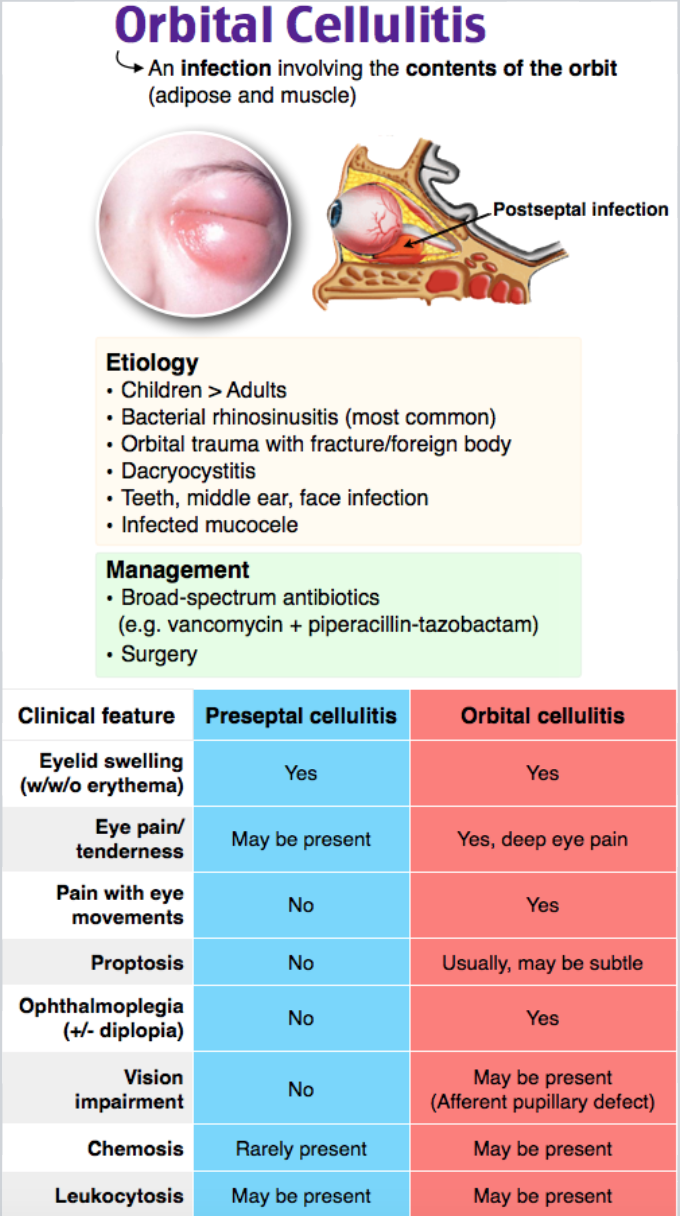
Orbital vs. Periorbital cellulitis
- Orbital cellulitis: occurs posterior to orbital septum within bony orbit
- Requires parental antibiotics +/- surgical drainage
- Periorbital cellulitis: more common, does not extend posterior to orbital septum, no change in visual acuity, conjunctival injection, proptosis, or intraorbital pathology7
- Outpatient management if patient is well-appearing; if toxic, admit
Clinical Presentation:
- Erythematous, edematous eye lids
- Suspect orbital cellulitis if any of the following present:
- Impaired or painful extraocular movements
- Decreased visual acuity
- Chemosis
- Proptosis
- Afferent pupillary defect7
- UK guidelines recommend admission is necessary if concerned for orbital cellulitis and any of the following presenting signs or symptoms:8
- Periorbital swelling, diplopia, reduced visual acuity, abnormal light reflexes, proptosis, ophthalmoplegia, drowsiness, vomiting, headache, seizures
Evaluation:
- Assess ABCs and obtain VS to include visual acuity
- Fever may or may not be present9
- Perform a complete physical examination
- Ocular: visual acuity, pupils, extraocular movements
- If patient cannot open eye, use ocular ultrasound to evaluate direct and consensual pupil reactivity
- Neuro: Focal neurologic deficits; CN III, IV, VI palsies
- ENT: dental exam to assess for deep space infections/dental infections; assess for concomitant ear infection, sinus infection
- Ocular: visual acuity, pupils, extraocular movements
- Imaging: CT sinus/orbits to evaluate orbital involvement, proptosis, periosteal reaction, sinus disease, foreign body
- Other indications for CT: focal CNS sign, no improvement over 24 hours, non-resolving pyrexia over 36 hours8
- Use of CT predicts accuracy of cases requiring surgical intervention10
- Laboratory evaluation:
- CBC with differential
- Nares culture, Conjunctiva culture
- Orbital cellulitis is a clinical diagnosis, but these may help narrow antibiotics
- Blood cultures are rarely positive2
- Nares culture, Conjunctiva culture
- LP: Consider in patient with fever, headache, focal neurologic deficit, or toxic appearance for meningitis
- CBC with differential
Treatment:
- ABCs—Toxic appearing patients require resuscitation.
- Concern for elevated ICP from abscess, etc., then consider treatments to reduce ICP (hyperosmotic therapy)11
- Antibiotics: 1-2 weeks IV, followed by outpatient therapy to complete a 4 week total course
- Empiric 1st line: 3rd generation cephalosporin or ampicillin/sulbactam12
- Suspicion of anaerobes: metronidazole, clindamycin, cefuroxime2
- 3rd generation cephalosporins, penicillin, and metronidazole have excellent CNS penetration13
- Add Vancomycin for life-threatening infections or if concerned for MRSA1,14
- Consult ophthalmology and/or ENT for evaluation
- Assess for abscess, may require drainage
- More common in older patients15
- Complications if inadequately treated:2
- Orbital abscess
- CVST
- Panophthalmitis
- Endophthalmitis
- Subperiosteal abscess
- Orbital compartment syndrome can result, causing permanent vision loss
- Assess for abscess, may require drainage
Pearls:
- LP if accompanied by fever, headache, neurologic symptoms, or toxic appearance
- CT aids in guiding surgical management
- Older children and adults are more predisposed to anaerobic infections often need both parenteral antibiotics and surgery—consider cefuroxime in these cohorts

An 18-year-old man presents to the emergency department with complaint of eye pain and eyelid swelling for three days. He denies any trauma to the area but had an upper respiratory infection recently. He endorses fevers and chills at home. His exam is notable for periorbital erythema and edema, intact extraocular eye movements, symmetrically reactive pupils, normal visual fields, and exacerbation of his pain on movement of his eyes. The contralateral eye is not involved. Which of the following is the most likely diagnosis?
A) Cavernous sinus thrombosis
B) Iritis
C) Orbital cellulitis
D) Periorbital cellulitis
Answer: C
Orbital cellulitis is an infection of the subcutaneous tissue and ocular muscles located inside the orbit. Extension of bacterial rhinosinusitis is the most common cause of orbital cellulitis. Orbital cellulitis must be distinguished from periorbital, or preseptal, cellulitis as periorbital cellulitis is typically a mild condition and orbital cellulitis is associated with a high risk of visual loss and mortality. Both may present with fever, eyelid swelling and redness, and ocular pain. Only orbital cellulitis will be associated with pain on movement of the eyes due to infection of the extraocular muscles, as well as proptosis, ophthalmoplegia, and diplopia. The presence of these symptoms should prompt imaging to evaluate for complications of orbital cellulitis, including cavernous sinus thrombophlebitis or abscess formation. Imaging studies may also aid in the diagnosis of orbital cellulitis if the diagnosis is uncertain. Orbital cellulitis is managed with admission and broad-spectrum intravenous antibiotic administration. Frequent visual checks and ocular examinations should be done as changes in the exam may signal the beginning of an abscess or extraorbital extension of the infection.
Cavernous sinus thrombosis (A) is a possible serious complication of extraorbital extension of orbital cellulitis. Clinical features to raise suspicion for this diagnosis include spread to the contralateral eye and dysfunction of the cranial nerves that pass through the cavernous sinus. Patients may present with ophthalmoplegia and gaze palsies of cranial nerves CN III, IV, or VI, and hypo- or hyperesthesia of the dermatomes innervated by cranial nerves V1 and V2. The patient above does not have any symptoms of extension of the infection into the cavernous sinus. Iritis (B) is inflammation of the uvea which includes the iris, ciliary body, and choroid. Symptoms of iritis vary and may include eye pain and redness with decreased visual acuity. Diagnosis is through visualization of leukocytes in the anterior chamber of the eye by slit lamp examination. Periorbital cellulitis (D) is infection of the soft tissues anterior to the orbital septum and does not cause pain on movement of the eye due to lack of involvement of the extraocular muscles.
FOAMed:
References:
- Wald ER. Periorbital and Orbital Infections. Infect Dis Clin North Am. 2007;21(2):393-408.
- Tsirouki T, Dastiridou AI, Cerpa JC, Moschos MM, Brazitikos P, Androudi S. Major review Orbital cellulitis. Surv Ophthalmol. 2018;63:534-553.
- Viet H. Ho MWWJCFBGH. Retained Intraorbital Metallic Foreign Bodies. Ophthalmic Plast &. 2004;20(3):232-236.
- Chaudhry IA, Shamsi FA, Elzaridi E, et al. Outcome of Treated Orbital Cellulitis in a Tertiary Eye Care Center in the Middle East. Ophthalmology. 2007;114(2):345-354.
- Tas S, Top H. Intraorbital wooden foreign body: clinical analysis of 32 cases, a 10-year experience. Turkish J Trauma Emerg Surg. 2014;20(1):51-55.
- Toumi A, Larbi Ammari F, Loussaief C, et al. Rhino-orbito-cerebral mucormycosis: Five cases. Médecine Mal Infect. 2012;42(12):591-598.
- Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline D. Tintinalli’s Emergency Medicine : A Comprehensive Study Guide.
- Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol Allied Sci. 2004;29(6):725-728.
- Nageswaran S, Woods CR, Benjamin DK, Givner LB, Shetty AK. Orbital Cellulitis in Children. Pediatr Infect Dis J. 2006;25(8):695-699.
- Le TD, Liu ES, Adatia FA, Buncic JR, Blaser S. The effect of adding orbital computed tomography findings to the Chandler criteria for classifying pediatric orbital cellulitis in predicting which patients will require surgical intervention. J Am Assoc Pediatr Ophthalmol Strabismus. 2014;18(3):271-277.
- Brook I. Microbiology and antimicrobial treatment of orbital and intracranial complications of sinusitis in children and their management. Int J Pediatr Otorhinolaryngol. 2009;73(9):1183-1186.
- American Academy of Pediatrics. Subcommittee on Management of Sinusitis and Committee on Quality Improvement. Clinical practice guideline: management of sinusitis. Pediatrics. 2001;108(3):798-808.
- Garcia G. Criteria for nonsurgical management of subperiosteal abscess of the orbit Analysis of outcomes 1988–1998. Ophthalmology. 2000;107(8):1454-1456.
- Prentiss KA, Dorfman DH. Pediatric Ophthalmology in the Emergency Department. Emerg Med Clin North Am. 2008;26(1):181-198.
- Harris GJ. Subperiosteal Abscess of the Orbit: Computed Tomography and the Clinical Course. Ophthalmic Plast &. 1996;12(1):1-8. https://insights.ovid.com/crossref?an=00002341-199603000-00001. Accessed January 5, 2019.




