Authors: Matthew R Levine, MD (Assistant Professor and Director of Trauma Services, Department of Emergency Medicine, Northwestern Memorial Hospital, Chicago, IL) and Lora Alkhawam, MD (Attending Physician, Duke Regional Hospital, Department of Emergency Medicine, Durham, NC) // Edited by: Erica Simon, DO, MHA (@E_M_Simon) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
An 85 year-old male is brought in by EMS status post MVC. He is confused and unable to detail the events surrounding his accident. When questioned, he has no recollection of his PMHx, but repeatedly states that he is in pain secondary to his c-collar and backboard. Vitals: HR 70 and irregular, BP 110/65, RR 16, O2 sat 94% on room air. Primary and secondary surveys are remarkable only for scant wheezing upon pulmonary auscultation. GCS is 14 without focal neurologic deficits. As you contemplate the next steps in your patient evaluation, you scan your knowledge bank: What critical diagnoses should you be considering? Let’s discuss some pearls and pitfalls in addressing the geriatric trauma patient.
Importance
According to 2010 US Census data, adults > 65 years of age account for 14% of the current U.S. population.1,2 It is estimated that nearly one in five Americans will be elderly by the year 2050.1,2 Why is this relevant to the practice of emergency medicine? Approximately 1 million persons aged 65 and older are affected by trauma each year.3 In fact, trauma in the elderly accounts for $12 billion in annual personal and institutional medical expenditures, and $25 billion in total annual healthcare expenditures.4 While elderly patients comprise a small percentage of total major trauma patients (8-12%) presenting to emergency care centers, they represent a disproportionate percentage of trauma fatalities and costs (15-30%).4
To date, numerous studies have demonstrated mortality related to trauma as increasing with advancing patient age.5-7 In fact, the Major Trauma Outcome Study published in 1989 (n = 3,833 > age 65 and 42,944 < age 65) demonstrated mortality as rising sharply between the ages of 45-55 and doubling by age 75.5 This pattern occurred at all Injury Severity Scores (ISS), mechanisms, and body regions.5
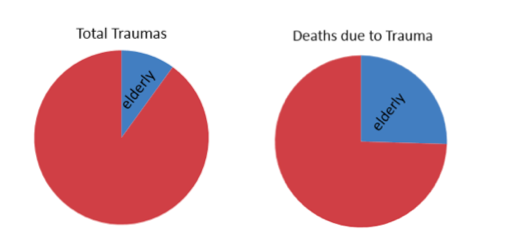
Representation of Trauma Mortality Data5
Today, we also know that advancing age is an independent risk factor for morbidity and mortality, despite lesser severity of injuries.1,2,5 However, while age has value in mortality projections for geriatric trauma patients presenting to the ED, literature suggests favorable functional outcomes for those who survive to hospital discharge.8 Therefore, age alone is not a criteria to deny or limit care in the elderly.9
Objectives
This review will highlight important differences in elderly trauma patients with respect to:
- Triage
- Pathophysiology in the Elderly
- Mechanisms and Patterns of Injury
- Trauma Bay Approach
- Special Considerations
There will be many citations throughout, but please keep in mind the limitations of research in geriatric trauma:8
- Few prospective randomized controlled trials
- No widely accepted age cut-off (“elderly” used to characterize patients ages 45-80)6
- Lack of a uniform definition of an elderly trauma patient
- Limited current studies (majority based in the 1980s-1990s)
Triage of the Elderly Trauma Patient
In its statement regarding trauma in the elderly, the CDC notes: “under triage of the older adult population is a substantial problem.”10 Under triage is defined as a failure to transport a trauma patient to a state-designated trauma center.10 Why is this important? Current studies (Zafar et al. and Maxwell et. al, 2015) have identified a significant mortality benefit for elderly patients presenting to trauma centers having had repeat exposure to geriatric trauma.11,12 Zafar et al. reported elderly patients as 34% less likely to die in these trauma centers.11 While it is true that level 1 trauma centers traditionally have longer lengths of stay and higher total costs of care, a large percentage of elderly trauma patients survive discharge from these facilities.11,12 Elderly patients with multiple injuries benefit from trauma center care.11,12 The difficulty here is that standard adult EMS triage guidelines provide poor sensitivity for detecting older adults that require trauma center care.13 The under triage rate is reported as 50%14,15 in patients older than 65, versus 17.8% for those under 65.14 Given this data, several experts have concluded that an age threshold should be established which mandates triage to a trauma center (various age ranges (55-70) have been recommended).6,9,16,17,18
What difficulties are encountered in identifying trauma severity in the elderly population? Potential explanations for under triage of elderly trauma patients are: significant injury secondary to low energy mechanisms, and altered physiologic response to injury with aging.
- The CDC recommends direct transport to a trauma center for any trauma patient age >65 with SBP <11010
- What affect does this have on triage of the elderly population? One that is substantial:
- Substituting SBP < 110 instead of SBP < 90 for patients older than 65 reduced under triage by 4.4%, while only increasing over triage by 4.3%.19
- What affect does this have on triage of the elderly population? One that is substantial:
Once an elderly patient arrives at a trauma center, trauma team activation occurs significantly less often for elderly patients (14% vs 29%) despite a similar percentage of severe injuries (defined as ISS>15).l
- The Eastern Association for the Surgery of Trauma (EAST) recommends a lower threshold for trauma team activation for patients 65 and older evaluated at trauma centers (level 3 evidence).20
- Some trauma centers use age as mandatory criteria for trauma team activation. This is supported by data that 63% of elderly trauma patients with ISS > 15 had no standard physiologic activation criteria.20
Clinical implications: Have a low threshold for recommending EMS transport of elderly trauma patients to a designated trauma center, especially for patients with SBP < 110. Have a low threshold for activating the trauma team for elderly trauma patients.
Pathophysiology Concerns in the Elderly
No other population is more susceptible to serious injury secondary to low-energy mechanisms (particularly falls) than the elderly. The elderly are less able to compensate for physiologic stresses occurring during injury, and are more likely to suffer complications during treatment and recovery. Key reasons for this are:
- Less physiologic reserve
- Occult shock/misleading picture of stability
- Comorbid illnesses (See Figure below)
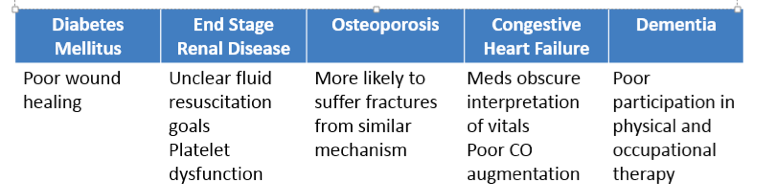
Comorbid Illnesses Contributing to Morbidity and Mortality in the Elderly
It is important to note that in elderly patients, profound shock may be present even in the setting of “normal” vital signs. Pharmaceutical therapy in the elderly (beta blockers and calcium channel blockers) may prevent typical tachycardic responses in shock states. Also significant, aging myocardium exhibits decreased sensitivity to endogenous catecholamines.
Blood pressures considered normal in young patients may represent hypotension when compared to baseline BPs in an elderly patient. A landmark article by Scalea et al. assessing early invasive (PA catheter) monitoring in elderly trauma patients demonstrated that the majority of trauma patients experienced profound perfusion deficits despite “normal” vital signs.19 In fact, a HR>90 and SBP<110 have been correlated with increased mortality in the elderly trauma population.19,21 What does this mean for the EM provider? The window to intervene may be narrow; delayed recognition of shock may postpone life-sustaining resuscitation.
What about additional markers of perfusion?
Multiple studies have demonstrated that elevated lactate levels (>2) or abnormal base deficit (<-6) are associated with major injury and mortality in trauma patients.23-25 One such study, performed in 1987, identified a venous lactate > 2.5 as a marker of occult hypoperfusion in 20% of the included geriatric patients.26 Lactate levels or ABG base deficit should be used as an adjunct to vital signs for early identification of perfusion deficits in elderly trauma patients.
Clinical implications: Avoid being falsely reassured by normal vital signs in elderly trauma patients. Use lactate levels or ABG with base deficit as adjuncts to vital signs to detect occult shock and guide resuscitation in unclear cases. Also use ECGs as an adjunct to detect silent ischemia as a response to the physiologic stress of trauma. Have a low threshold for admitting elderly trauma patients to an ICU.
Mechanisms and Patterns of Injury
Which mechanisms and patterns of injury are more concerning in the elderly? They all are.
More specifically, falls from ground level, head trauma, chest wall injuries, pedestrian struck by vehicle, and cervical spine injuries have a disproportionate burden on elderly patients.
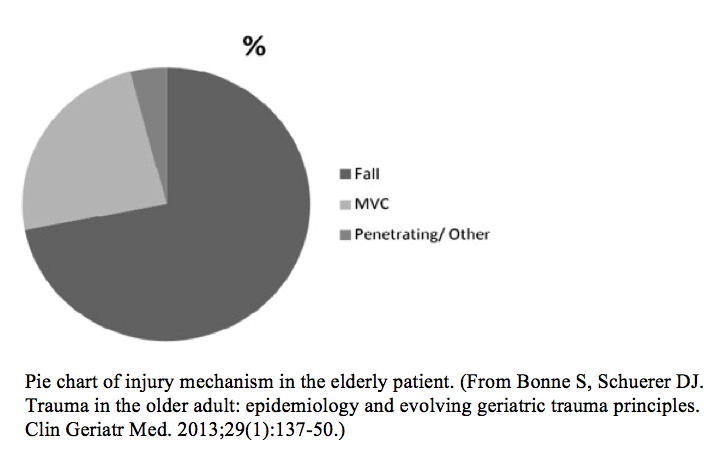
Falls are the most frequent cause of injury in patients > 65 years of age, and are the most common fatal accident in patients > 80 years of age.27 More than one third of elderly patients presenting to the ED post fall return to the ED, or die within one year of initial evaluation.28 Same level falls must not be minimized – they are ten times more likely to cause death in an elderly vs. non-elderly patient (25% vs 2.5%).29 Even falls that seem purely mechanical can be a sign of occult illness. It is imperative that emergency physicians perform a complete H&P for all elderly patients having experienced a fall for:
- Sudden disturbances in cardiovascular/neurologic function
- New/progression of underlying conditions or emerging infection
- Intoxicants/medication effects
- Environmental safety
- Impact of injury on functional status/ability to care for self
Why are falls so devastating in the elderly population?
Age-related atrophy of the brain leads to increased potential space and shearing forces on the intracranial bridging veins when exposed to trauma. The risk of intracranial bleeding is also markedly increased with medications commonly prescribed to the elderly (anticoagulants and anti-platelets).30,31 Keep in mind that older patients are excluded from studies that attempt to identify populations in which imaging is low yield = IMAGE the elderly.
Outside of head trauma, are there any other areas for EM docs to be on the lookout?
Even “minor” chest injuries impair the elderly. Thoracic cage trauma is poorly tolerated secondary to decreased compliance, loss of alveolar surface area, impaired lung defenses, and increased pulmonary bacterial colonization with aging. A rigid C-collar and backboard can further impair chest wall expansion. Elderly patients with rib fractures are at increased risk for pneumonia (31% vs. 17% with 16% increase per rib fractured), pulmonary contusion, and delayed hemothorax.32 Mortality also increases 19% per rib fractured.32
The elderly spine is vulnerable to fracture from minor mechanisms due to conditions such as cervical stenosis, osteoporosis, and degenerative, rheumatoid, and osteoarthritis.33 High cervical fractures (type 2 odontoid being the most common), and central cord syndromes are also more frequent in the elderly.34
Pedestrian struck by a vehicle is perhaps the most devastating mechanism of injury to disproportionately affect this population. Patients age > 65 account for 22% of pedestrian vs. MVC deaths.33 Current statistics report 46% of these accidents as occurring in crosswalks.33 Factors that predispose the elderly to increased severity of injury include decreased ability to raise or turn the head due to cervical arthropathy, and reduced speed and agility (crosswalk timers often allow for a pedestrian speed of 4 ft/sec).33
Clinical implications: Maintain a heightened suspicion for significant injury (especially intracranial and C-spine pathology) even from ground level falls. Assess elderly patients for medical impairments that may have precipitated the fall. Be liberal with CT scanning for elderly head and neck trauma, and always inquire regarding the use of anticoagulant and antiplatelet medications. Ensure adequate analgesia and oxygenation for chest wall injuries. Remove the collar and backboard as early as safely possible. Maintain a low threshold for admitting elderly patients with rib fractures.
Special Considerations
ABCs in the Elderly
- A – Early airway control. Edentulous patients may be difficult to bag; remove dentures for intubation.
- B – Avoid respiratory decompensation by use of O2; analgesia for chest injuries; suction/pulmonary toilet; clear the C-spine, and remove the backboard as early as possible to prevent respiratory impairment.
- C – Early transfusion to minimize fluid overload from crystalloids. Recognizing that “normal” BP may be relative hypotension for an elderly patient. Question patients regarding anticoagulant use and consider reversal early in the course.
- D – Liberal use of head and C-spine CT; GCS is not a sensitive indicator in the elderly trauma patient.
- E – Assess for signs of comorbidities that may not have been reported (i.e. surgical scars, pacemakers, medications or med lists in patient belongings, medical alert tags, bruising from anticoagulants).
Elder Abuse
No report on elderly trauma is complete without mention of elder abuse. Elder abuse can be very difficult to detect for several reasons:
- Patient reluctance to identify a loved one
- Patient dependence on the abuser
- Perceived frailty limiting the patient from feeling empowered in seeking help
- Patient mental or memory impairment limits the history
- Abuse in the form of neglect can mimic cachexia from comorbidities
Clinical implications: When the scenario has stabilized, assess the patient’s social situation. Be wary of wounds or injuries that are suspicious for abuse or do not match the reported mechanism of injury. And of course, ask the patient, preferably in private!
A Quick Word on Anticoagulants
Anticoagulant use is far more prevalent in the elderly population. An increasing portion of the elderly population are being prescribed novel oral anticoagulants, which are not as readily reversible as warfarin. An elderly trauma patient should be questioned regarding anticoagulants ASAP. An irregular heartbeat may be a clue to chronic atrial fibrillation and anticoagulant use. Know your institution’s reversal protocol for the novel anticoagulants. If your institution does not have a protocol, then have a plan in mind. Know which prothrombin complex concentrates are available to you. Know if Praxbind is stored by your pharmacy.
Back to the Case
The patient in the initial case presentation may have been exhibiting his normal baseline mental status or could have been confused secondary to the emotional distress pertaining to the accident, but the provider must assume the confusion secondary to intracranial bleeding until proven otherwise. The patient’s irregular heart rate should alert the clinician to the possibility of aspirin or anticoagulant use, necessitating a plan for reversal should it be needed. In terms of the rest of the vital signs: the patient’s “normal” blood pressure may actually represent relative hypotension. The borderline hypoxia (and wheezing discovered on exam) is likely related to lung injury, aspiration, or an underlying comorbidity (i.e. COPD or CHF). This should serve as a warning – the patient is high risk for respiratory decompensation from chest injury and impaired chest wall motion from the C-collar and backboard. The backboard should be removed as soon as possible, pain from the chest injury treated as applicable, and supplemental oxygen employed. Suction may be considered as an adjunct. If and when the C-spine is cleared, the patient should be placed in an upright position to facilitate gas exchange and decrease work of breathing. The patient may have critical injuries and blood loss despite minimal symptoms so a lactate or ABG for base deficit should be sent. Imaging to rule out internal injuries is a must. Initial diagnostic work-up and resuscitation should be aggressive until the patient’s prognosis and wishes are clear. Volume resuscitation should be minimized, with blood products being the fluid of choice. The clinician should have a low threshold for trauma team activation vs. consultation and admission.
Summary
- Resuscitation of the elderly trauma patient must be thoughtful but aggressive:
- Heighten awareness that with age, signs and symptoms may be minimal, and that the outcome is often initially unclear, and commonly, but not necessarily poor.
- Up to 85% of elderly trauma survivors return to baseline or independent function.9
- This justifies initial aggressive approach which can be reassessed later when patient/family wishes and prognosis becomes increasingly clear.9
- Less physiologic reserve leaves little time for delays in diagnosis and under- or over- resuscitation.
- Blood is the fluid of choice.
- The principles of diagnosis and management in trauma are the same regardless of age, but the incidence of physiologic changes and disease states mandates a different overall approach.
- You may be the only one in the room who knows how sick the patient really is.
References / Further Reading
- Hashmi A, Ibrahim-Zada I, Rhee P et al. Predictors of mortality in geriatric trauma patients: A systematic review and meta-analysis. J Trauma Acute Care Surg. 2014;76:894-901.
- Vincent GK, Velkoff VA, U.S. Census Bureau. The next four decades the older population in the United States: 2010 to 2050. Population estimates and projections P25-1138. Washington, DC: U.S. Dept. of Commerce, Economics and Statistics Administration, U.S. Census Bureau; 2010. Available from http://purl.access.gpo.gov/GPO/LPS126596.
- CDC National Center for Health Statistics (NCHS), National Vital Statistics System. http://www.cdc.gov/nchs/nvss.htm.
- CDC Data and Statistics (WISQARSTM): Cost of Injury Reports Data Source: NCHS Vital Statistics System for Numbers of Deaths. http://wisqars.cdc.gov/8080/costT/.
- Champion HR, Copes WS, Buyer D et al. Major trauma in geriatric patients. Am J Public Health. 1989;79:1278-1282.
- Bonne S, Schuerer D. Trauma in the Older Adult – Epidemiology and evolving geriatric trauma principles. Clin Geriatr Med. 2013;29:137-150.
- Goodmanson NW, Rosengart MR, Barnato AE et al. Defining geriatric trauma: When does age make a difference? Surgery. 2012;152:668-675.
- Grossman MD, Ofurum U, Stehly CD et al. Long-term survival after major trauma in geriatric trauma patients: The glass is half full. J Trauma. 2012;72:1181-1185.
- Jacobs DG, Plaisier BR, Barie PS et al. Practice Management Guidelines for Geriatric Trauma. The EAST Practice Management Guidelines Work Group. J Trauma. 2003;54:391-416.
- Sasser SM, Hunt RC, Faul M et al. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR Recomm Rep. 2012 Jan 13;61(RR-1):1-20.
- Zafar SN, Obirieze A, Schneider EB et al. Outcomes of trauma care at centers treating a higher proportion of older patients: The case for geriatric trauma centers. Acute Care Surg. 2015;78:852-859.
- Maxwell CA, Miller RS, Dietrich MS et al. The aging of America: a comprehensive look at over 25,000 geriatric trauma admissions to United States hospitals. Am Surg. 2015;81(6): 630-636.
- Ichwan B, Subrahmanyam D, Shah MN et al. Geriatric-specific triage criteria are more sensitive than standard adult criteria in identifying need for trauma center care in injured older adults. Ann Emerg Med. 2015;65:92-100.
- Chang DC, Bass RR, Cornwell EE et al. Undertriage of elderly trauma patients to state-designated trauma centers. Arch Surg. 2008;143:776-781.
- Kodadek LM, Selvarajah S, Velopulos CG et al. Undertriage of older trauma patients: is this a national phenomenon? J Surg Research. 2015;199:220-229.
- Caterino JM, Valasek T, Werman HA. Identification of an age cutoff for increased mortality in patients with elderly trauma. Am J Emerg Med. 2010;28:151-158.
- Lehmann R. The impact of advanced age on trauma triage decisions and outcomes: a statewide analysis. Am J Surg. 2009 May; 197(5):571-4.
- American College of Surgeon Committee on Trauma. Geriatric Trauma. In: ATLS: student course manual. 8th Chicago. 2008:247-257.
- Scalea TM, Simon HM, Duncan AO et al. Geriatric blunt multiple trauma: improved survival with early invasive monitoring. J Trauma. 1990; 30: 129–136.
- Brown JB, Gestring ML, Forsythe RM et al. Systolic blood pressure criteria in the National Trauma Triage Protocol for geriatric trauma: 110 is the new 90. J Trauma Acute Care Surg. 2015;78:352-359.
- Calland JF, Ingraham AM, Martin N et al. Evaluation and management of geriatric trauma: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:S345-S350.
- Heffernan DS,Thakkar RK, Monaghan SF, et al. Normal presenting vital signs are unreliable in geriatric blunt trauma victims. J Trauma. 2010;69(4):813-820.
- Zehtabchi S, Baron BJ. Utility of base deficit for identifying major injury in elder trauma patients. Acad Emerg Med. 2007;14:829-831.
- Callaway DW, Shapiro NI, Donnino MW et al. Serum lactate and base deficit as predictors of mortality in normotensive elderly blunt trauma patients. J Trauma. 2009;66:1040-1044.
- Paladino L, Sinert R, Wallace D et al. The utility of base deficit and arterial lactate in differentiating major from minor injury in trauma patients with normal signs. Resuscitation. 2008;77:363-368.
- Salottolo KM, Mains CW, Offner PJ et al. A retrospective analysis of geriatric trauma patients: venous lactate is a better predictor of mortality than traditional vital signs. Scan J Trauma Resusc Emerg Med. 2013;21:1-7.
- Labib N,Nouh T, Winocour S et al. Severely injured geriatric population: morbidity, mortality, and risk factors. J Trauma. 2011;71(6):1908-14.
- Liu SW, Obermeyer Z, Chang Y et al. Frequency of ED revisits and death among older adults after a fall. Am J Emerg Med. 2015;33:1012-1018.
- Sterling DA,O’Connor JA, Bonadies J. Geriatric Falls: injury severity is high and disproportionate to mechanism. J Trauma. 2001;50(1):116-119.
- Rathlev NK, Medzon R, Lowery D et al. Intracranial pathology in elders with blunt head trauma. Acad Emerg Med. 2006;13(3):302-7.
- Li J, Brown J, Levine M. Mild head injury, anticoagulants, and risk of intracranial injury. Lancet. 2001; 357(9258):771-2.
- Bulger EM. Rib fractures in the elderly. J Trauma. 2000;48(6):1040.
- Bonne S, Schuerer DJ. Trauma in the older adult: epidemiology and evolving geriatric trauma principles. Clin Geriatr Med. 2013;29(1):137-50.
- Reinhold M, Bellabarba C, Bransford R et al. Radiographic analysis of type II odontoid fractures in a geriatric patient population: description and pathomechanism of the “Geier”-deformity. Eur Spine J. 2011. Nov;20(11):1928-39







2 thoughts on “Geriatric Trauma and Medical Illness: Pearls and Pitfalls”
Pingback: Länkar v35 | Internmedicin