
Authors: Alin Gragossian, DO and Alex Asp, MD (Emergency Medicine Residents at Drexel University, Department of Emergency Medicine) and Richard Hamilton, MD (Emergency Medicine Chair at Drexel University, Department of Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
Case Presentation
A 34-year-old female is brought by EMS in respiratory distress with audible wheezing. Per EMS, she has a history of hypertension, asthma, and medication noncompliance. The patient is unable to provide any history. Initial vitals in the emergency department include BP 152/80, HR 120, RR 32, SpO2 87% on room air, T 99.0°F.
The patient is using accessory muscles to breathe and appears anxious. She has expiratory wheezes bilaterally with decreased inspiratory sounds. EMS tells you she was given two doses of nebulized albuterol en route with minimal relief of her symptoms. You ask your nurse to give her 125 mg methylprednisolone intravenously and 3ml of nebulized albuterol/ipratropium repeated x 3. You also ask for the patient to be placed on BiPAP, but there is no machine immediately available so the respiratory technician has to get one from the ICU. As you are waiting for the machine, the patient begins to tire, so you decide to intubate her. A delayed sequence intubation is undertaken with 1 mg/kg ketamine intravenously as the induction agent. To preoxygenate/denitrogenate, you provide positive airway pressure by applying bag valve mask with PEEP valve set at 10 cmH2O, two hand seal, max flow nasal cannula, and allow the patient to spontaneously ventilate. The pulse oximeter improves to 99%, and you administer 1.2 mg/kg rocuronium, wait for paralysis, and intubate with a 7.5 cm tube without complications. The respiratory technician returns and grabs the ventilator, and the initial settings include:
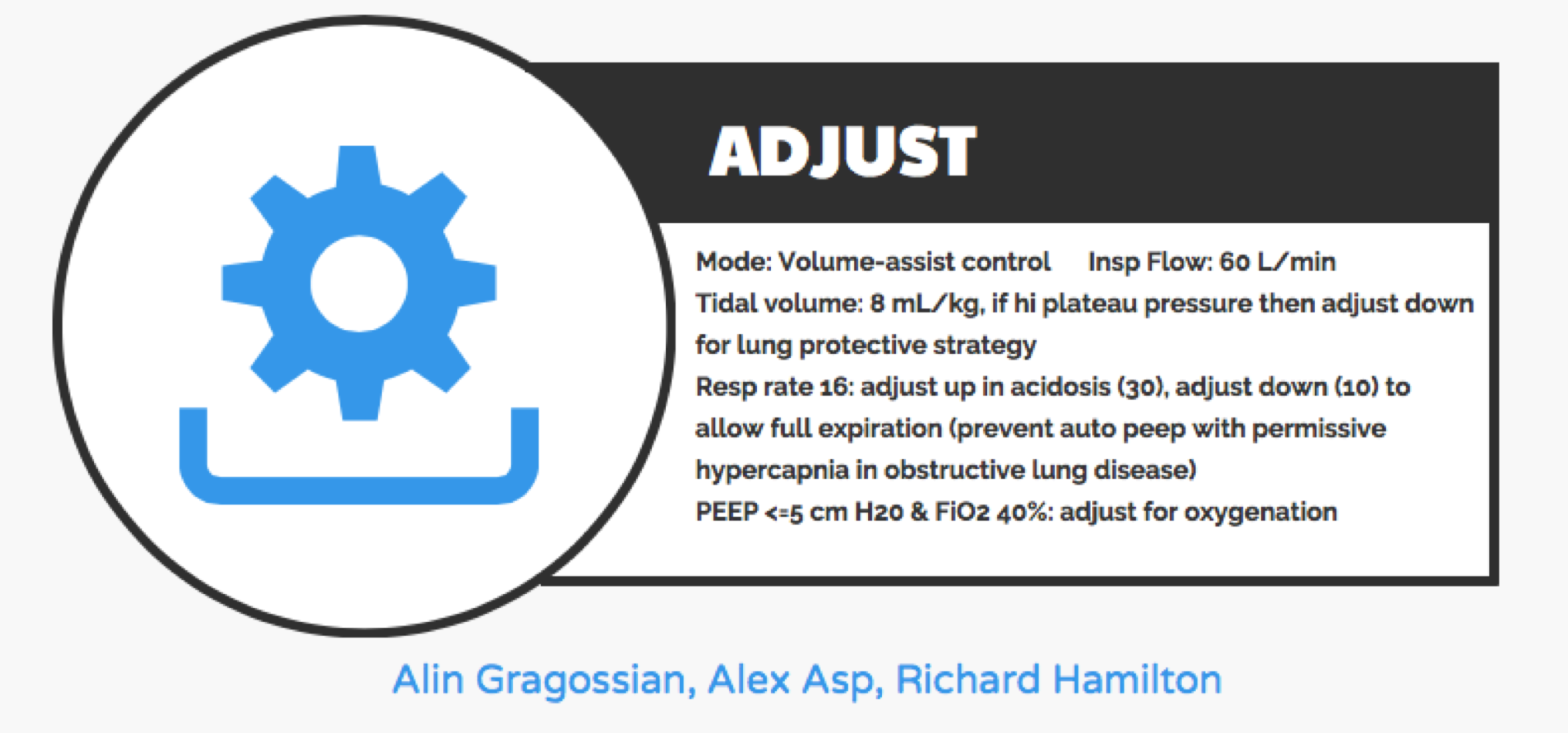
Mode: Volume Assist Control
TV: 450 (8 ml/kg IBW)
RR: 18
FiO2: 100%
PEEP: 5
I:E ratio of 1:2
You get called back into the room thirty minutes later because the ventilator is alarming for increased peak airway pressures. Repeat vitals include BP 90/62, HR 130, RR: 18, SpO2 89% on 100% FiO2.
You stop and think about what is going on, and you remember that asthmatics are at risk for crashing once on the mechanical ventilator. In fact, many of the patients we intubate in the ED are at high risk for significant cardiopulmonary complications after intubation. This post will evaluate several populations who may decompensate with intubation, while providing pearls in management.
Obstructive Airway Disease
The pathophysiology underlying obstructive airway disease (in particular, asthma and COPD) includes inflammation, hypersecretion of mucus, and bronchoconstriction that limit airflow, especially during expiration. This causes trapping of air that is high in CO2 and low in O2. When intubating/ventilating these patients, the following considerations have to be made:
- Expiration is impaired, so longer time for exhalation is required
- Trapping of air causes a buildup of pressure in the chest, decreasing preload
Danger with intubation/ventilation
Failure to account for the longer required expiratory time prevents the lungs from emptying between breaths, which in turn causes trapping of air and retention of CO2, often called “breath-stacking”. When this occurs, the volume in the lungs increases with each delivered breath since the volume from the ventilator is constant, and there is progressively more volume retained in the lungs. The increased volume leads to increased intrapulmonary pressure, called intrinsic positive-end-expiratory pressure (i-PEEP) or auto-PEEP, which contributes to barotrauma such as pneumothorax, interstitial emphysema, and pneumomediastinum. It can also cause parenchymal lung injury, including ARDS1. Lastly, increased intrapulmonary pressure causes increased intrathoracic pressure, which can impair filling of the heart (decreased preload) and lead to hypotension.
How to prevent crashing with intubation
- Consider ketamine2 or propofol3 as the induction agent
- Both have bronchodilatory effects
- Consider rocuronium as the paralytic
- Longer paralysis time can help with vent synchrony
- Use a larger endotracheal tube
- Use low tidal volumes – 6-8 ml/kg IBW
- Decrease respiratory rate – start with 10 bpm
- Decrease I:E ratio – 1:3–1:5
- Consider heliox – asthma only
- Heliox is oxygen mixed with helium instead of nitrogen (room air), creating a mixed gas that has a lower density. Some studies have shown that it can decrease airway resistance and improve outcomes in patients with asthma (but not COPD), but studies have been limited4,5. If using heliox in a ventilated patient, make sure to adjust settings carefully, as some ventilators will require pressure-cycle rather than volume-cycle1.
- Consider disconnecting from ventilator and pushing on the chest if patient is breath-stacking
How to monitor for success
- High peak airway pressure (PIP) is better tolerated than high plateau pressure. High plateau pressure reflects alveolar pressure and causes lung injury if it is above 30 cmH2O. Therefore, maintain plateau pressure <30 cmH2O by reducing respiratory rate. You will likely need to reset the alarm for high PIP to ensure the ventilator continues to provide breaths.
- Accept mild hypercapnia and acidemia.
Metabolic Acidosis
In metabolic acidosis, there is compensatory hyperventilation to attempt to preserve physiologic pH by decreasing pCO2. The patient’s capacity to compensate is very high, so if that compensation is taken away, they will, theoretically, rapidly deteriorate due to worsening acidosis6. There are many disease states where a patient is heavily reliant upon hyperventilation to maintain pH. The most common are:
- Diabetic ketoacidosis (DKA)
- Lactic acidosis (sepsis, mesenteric ischemia, severe anemia)
- Salicylate toxicity
Danger with intubation/ventilation
In these patients, there are two main dangers: the period of apnea during the intubation and the ventilatory rate. Paralyzing for intubation causes a transient increase in pCO2 that is normally clinically insignificant, but in the already acidotic patient who had been compensating, this further insult can cause cardiovascular collapse. Once on the ventilator, the patient will initially be paralyzed so the set respiratory rate will be their actual rate, and they will have no intrinsic ability to compensate for their acidosis.
How to prevent crashing with intubation
- Optimize cardiovascular status before intubating – Provide IV fluids and vasopressors if needed
- Use noninvasive ventilation such as BiPAP for pre-oxygenation
- Avoid apnea if at all possible by using a delayed sequence technique with ketamine as induction agent to allow patient to spontaneously ventilate
- Consider shorter acting paralytic such as succinylcholine
- Increase respiratory rate to 30 – or at least match the patient’s rate before intubation
- Use tidal volume closer to 8 ml/kg IBW
How to monitor for success
- Check frequent arterial or venous blood gases with ventilator setting adjustments
Shock
Critically-ill patients are at increased risk for hypotension while being mechanically ventilated7. Patients may be compensating for hypotension through negative-pressure breaths, helping to draw blood back to the heart.
Danger with intubation/ventilation
Once positive pressure ventilation (PPV) is initiated, the pulmonary veins and vena cava are compressed, and the decreased venous return can worsen underlying shock. Distributive shock from causes such as sepsis and anaphylaxis is the result of decreased systemic vascular resistance, making the patient more susceptible to PPV-induced hypotension5. Hemorrhagic shock can also worsen with PPV due to decreased volume to overcome vascular compression.
How to prevent crashing with intubation
- Fluid resuscitate prior to intubation
- Begin vasopressors prior to intubation, if needed5
- Have bolus doses of vasopressor at bedside, for example 5 to 20 mcg boluses of epinephrine
- Lower the dose of etomidate8,9 or ketamine10 as the induction agent by 50%, and use the highest dose of paralytic (shock states mean preferred blood flow to CNS [induction agent] but lower flow to muscles/motor end plate [paralytic]). Propofol can be used at a lower dose (again, < 50%), but beware its hypotensive effects
- Lower PEEP to decrease intrathoracic pressure
How to monitor for success
- Repeat blood pressure measurements frequently after intubation
- Place an arterial line if requiring vasopressors
Pulmonary Hypertension
Pulmonary hypertension causes chronic right heart strain, and patients can deteriorate quickly from multifactorial cardiopulmonary decompensation.
Danger with intubation/ventilation
Positive pressure ventilation increases intrathoracic pressure and causes compression of the right atrium, reducing preload1. In chronic pulmonary hypertension, decreased preload and increased afterload can quickly lead to cardiovascular collapse11. Patients with pulmonary hypertension and systemic hypotension may worsen with intravenous fluids due to over-distension of the strained right ventricle11.
How to prevent crashing with intubation
- Consider pre-medicating with fentanyl to blunt the hypertensive response to laryngoscopy5
- Consider etomidate8,9 as the induction agent
- Use low tidal volume – 4-6 ml/kg IBW
- Lower PEEP
How to monitor for success
- Maintain plateau pressure < 30 cmH2O
- Check frequent blood gases to monitor for hypercapnia
- These patients are not candidates for permissive hypercapnia since acidemia causes vasoconstriction, increasing pulmonary arterial pressure11
- Avoid hypoxemia since this also causes vasoconstriction and worsens right ventricular afterload13
Case Resolution
You arrive at the bedside and see the peak pressure is 60 cmH2O. You ask the respiratory technician to measure a plateau pressure, and it is 45 cmH2O. You immediately disconnect the patient from the ventilator and hear a rush of air from the endotracheal tube. You begin manually bagging the patient at a slower rate, and the blood pressure and SpO2 improve. You place the patient back on the ventilator but adjust the settings as follows:
TV: decrease to 350 ml (6 ml/kg IBW)
RR: decrease to 10 bpm
Peep: 0 cm H2O
I:E ratio: decrease to 1:4
The patient remains stable and is transported to the ICU without further issue.
Further Reading: A Summary of EMCrit’s “The Crashing Ventilated Patient”
The above post was specifically about scenarios based on critically ill patients’ disease pathophysiology. But, what do you do when any patient crashes while on the ventilator? We have taken the following tips from EMCrit (from https://emcrit.org/wp-content/uploads/2013/08/The-crashing-ventilated-patient_EMCrit-Conference.pdf)
A Patient with Hemodynamic and Ventilator Collapse
Diagnosing the Problem
- Use “D.O.P.E.S.”
- Displacement of ETT, cuff adjustment
- Obstructed tube
- Pneumothorax
- Equipment malfunction
- Stacking (“breath-stacking” or “auto-PEEP” as explained above)
Treating the Problem
- Use “D.O.T.T.S.”
- Disconnect the patient from the vent
- Oxygenate (use BVM on 100%)
- Tube position (reposition the ET tube)
- Tweak the ventilator settings (especially if auto-PEEP is suspected)
- Sonogram (ultrasound the lungs to r/o pneumothorax)
A Patient with Hemodynamic and Ventilator Collapse
- First, do the “quick check”
- Patient biting the tube
- Check vent connections
- Then, think back – “focused H&P”
- Who intubated? Were there any complications?
- What meds were used?
- What are the current oxygen saturations & ETCO2? What is the ABG?
- Have you checked for PTX?
- Waveform analysis
- Is there evidence of auto-PEEP?
- If so, perform an end-expiratory hold to determine autoPEEP
- Respiratory Mechanics
- Evaluate if the problem is due to resistance or compliance
- Evaluate peak pressure & plateau pressure. Find the difference between the two measures.
- If low, the problem is likely due to a compliance issue
- If high, the problem is likely due to a resistance issue
- Consider bronchoconstriction, dislodged ET tube, biting tube, mucus plug in tube
- Evaluate peak pressure & plateau pressure. Find the difference between the two measures.
- Evaluate if the problem is due to resistance or compliance
- Is there evidence of auto-PEEP?


Key Takeaways
- Not all induction agents and paralytics are equal
- Obstructive lung disease – use ketamine and longer-acting paralytic
- Metabolic acidosis – use shorter-acting paralytic
- Shock – use etomidate or ketamine at half dose and max dose of paralytics
- Pulmonary hypertension – use etomidate
- Decrease I:E ratio in obstructive airway disease
- Optimize hemodynamics with IV fluids and vasopressors before intubation and be ready for push doses of vasopressors immediately after intubation
- Permissive hypercapnia is acceptable in obstructive lung disease but NOT in pulmonary hypertension
- Check frequent blood gases on patients at high risk of decompensating after intubation
This post is sponsored by www.ERdocFinder.com, a supporter of FOAM and medical education, who with their sponsorship are making FOAM material more accessible to ER physicians around the world.

References/Further Reading:
- Arbo JE, Ruoss SJ, Lighthall GK, Jones MP, eds. Decision Making in Emergency Critical Care: An Evidence-Based Handbook. Philadelphia: Wolters Kluwer Health; 2015.
- Hemmingsen C, Nielson PC, Odorico J. Ketamine in the treatment of bronchospasm during mechanical ventilation. Am J Emerg Med. July 1994;12(4):417-420.
- Eames WO, Rooke GA, Wu RS, Bishop MJ. Comparison of the effects of etomidate, propofol, and thiopental on respiratory resistance after tracheal intubation. Anesthesiology. June 1996;84(6):1307-11.
- Hurford WE. Respiratory controversies in the critical care setting. Should heliox be used for mechanically ventilated patients? Respiratory care. May 2007;52(5):582-591.
- Ho AM, Lee A, Karmakar MK, Dion PW, Chung DC, Contardi LH. Heliox vs air-oxygen mixtures for the treatment of patients with acute asthma: a systematic overview. Chest. 2003;123(3):882-90.
- Mosier JM, Joshi R, Hypes C, Pacheco G, Valenzuela T, Sakles JC. The Physiologically Difficult Airway. West J Emerg Med. 2015;16(7):1109-17.
- Green RS, Edwards J, Sabri E, et al. Evaluation of the incidence, risk factors, and impact on patient outcomes of postintubation hemodynamic instability. CJEM. 2012;14:74-82.
- Ebert TJ, Muzi M, Berens R. Sympathetic responses to induction of anesthesia in humans with propofol or etomidate. Anesthesiology. 1992;76:725-33.
- Tassani P, Martin K, Janicke U, et al. Bolus administration of eltanolone, thiopental, or etomidate does not affect systemic vascular resistance during cardiopulmonary bypass. J Cardiothoracic Vasc Anesth. 1997; 11:562-4.
- Van Berkel MA, Exline MC, Cape KM, et al. Increased incidence of clinical hypotension with etomidate compared to ketamine for intubation in septic patients: a propensity matched analysis. Journal of Critical Care. 2017;38:209-214.
- Dalabih M, Rischard F, Mosier JM. What’s new: the management of acute right ventricular decompensation of chronic pulmonary hypertension. Intensive Care Med. 2014;40(12):1930-3.
- Hoeper M, Ganton J. Intensive care unit management of patients with severe pulmonary hypertension and right heart failure. Am J Resp Crit Care 2011; 184 (10): 1114-1124.
- Rudolph AM and Yuan S. Response of the pulmonary vasculature to hypoxia and H+ ion concentration changes. J Clin Invest. 1966;45:399-411.






2 thoughts on “High Risk Post Intubation Patients”
Pingback: emDOCs.net – Emergency Medicine EducationEM Educator Series: The High-Risk Intubation (Peri- and Post-intubation) - emDOCs.net - Emergency Medicine Education
Pingback: January ’19 Asynchronous Learning – Lakeland Health EM Blog