Time 12:25
Triage Note: 35M referred from Coumadin clinic for headache, dizziness and weakness.
Triage Vitals: BP 89/53 HR 89 RR 19 T 95.6 (oral) O2 98% Pain 5/10 (headache)
Time 13:40
Intern HPI
35M Jehovah’s witness with PMH of aortic valve repair at age 9 and aortic arch replacement 2 weeks ago at OSH for aortic aneurysm with dissection. Sent from Coumadin clinic for lightheadedness and headache. +dull headache and progressive lightheadedness x 2 days. His INR was 2.7 and Hbg 10mg/dL a few days ago. Denies active chest pain, palpitations, SOB, fever, head trauma. He has had significant weight loss since hospitalization.
- PMHX: prosthetic valve, aortic dissection s/p repair 2 weeks ago
- Meds: Coumadin, Metoprolol, Cozar, ASA
- ROS: otherwise negative
- Allergies: none
Exam
- Vitals: BP 93/52 HR 87 RR 16, 98% on RA
- Gen: Well-developed male
- HEENT: Pale conjunctiva and dry mucous membranes, OP clear
- Cardiac: RRR, valvular click, pulses equal bilaterally
- Lungs: CTAB, no wheeze or crackles. Surgical scar c/d/i
- Abd: Soft abdomen no masses
- Neuro: CN intact, strength equal bilateral
Labs
- Hbg 5.7
- INR 3.60
CXR
Sternotomy wires, no effusions, no pneumothorax or infiltrate
FAST
Negative
Assessment/Plan
35M s/p recent aortic arch repair, with supra-therapeutic INR, now with 2-3 days of lightheadedness on standing, increasing fatigue, and SBP of low 90s, concerning for anemia or hemorrhage 2/2 post-op cardiovascular pathology.
- ECHO
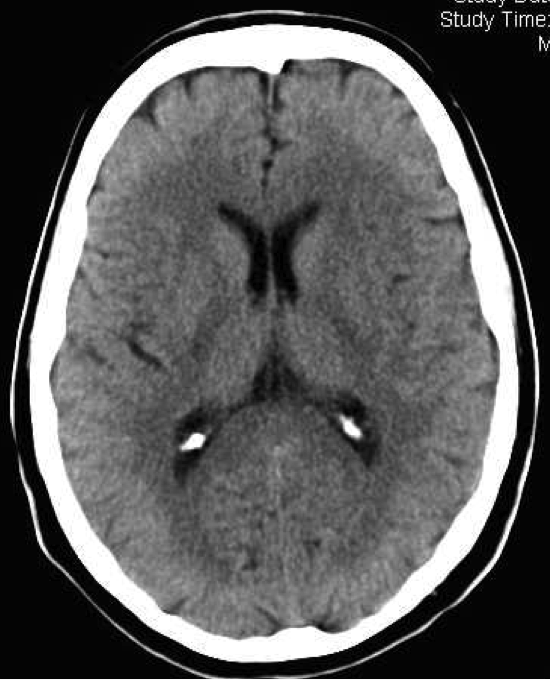
- HEAD CT
- CHEST CT
- CT Surgery Consult
Time 15:02
ECHO being performed. Tentative results: No bleeding source; AV function WNL; graft intact; EF WNL; no effusions; no dissection
Time 16:40
Head CT nml
Time 17:08
CTA Chest and Abdomen: no evidence of active extravasation/mediastinal hematoma. Multiple vascular embolization coils in abdomen.
Time: 17:40
(5 hours and 15 minutes since triage)
Rectal Exam done. Bright red blood in vault.
Time 17:59
Attending Update Note: CT head (for HA) negative; CT chest to look for aortic graft leakage negative. + guaiac noted-possible blood loss is in GI tract . GI consulted 1746. Patient has acute life threat risk from bleeding, He is a Jehovah’s Witness and refuses blood or blood products even if he might die without them. Critical need to localize the bleeding site and if GI have scope or IR stop bleeding.
Time 18:09
Nexium 80mg in 100ml NS over 30 minutes
Time 19:05
Admitting Resident’s Plan
- GI: EGD patient in ICU ASAP; continue Nexium gtt; 1L NS bolus; defer serial CBCs; patient refusing all blood/synthetic products; will consult Heme re: possible reversal agents ddAVP? Tranexamic acid? Bebulin?; spoke with Critical Care fellow via phone, aware of pt; holding off transfer to ICU given no opportunity to intervene
- CV: aggressive fluid resuscitation with NS; HR management diltiazem gtt if necessary; INR supra-therapeutic – will hold anticoagulation given acute bleed
- PPX: Nexium gtt; scds
- Dispo: to ICU; FULL CODE; NO BLOOD PRODUCTS
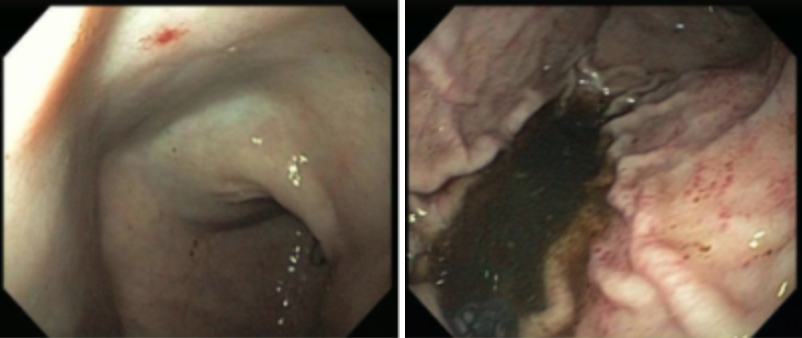
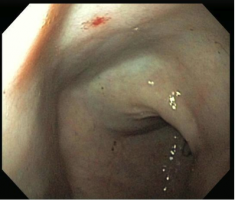
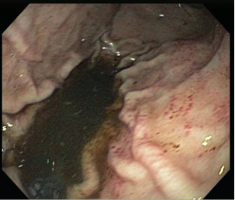
Esophagogastroduodenoscopy (EGD)
Teaching Points
Look early for all possible reversible causes of hypotension.
- In this case, GI bleed was only considered 5 hours after arrival to the ED.
- On further history patient reports that stool was newly JET black and STICKY for several days
Think about possible reversal or correction agents in patients who cannot accept human-donor blood products.
- Vitamin K, TXA, ddAVP, Protamine, PPI, Aprotinin for hemorrhage
- Iron, Folate, B12, Erythropoietin for anemia
- This patient received 5mg IV Vit K to reduce INR to 2. ddAVP was also given 2/2 hx of aspirin use.
Speak with Jehovah’s Witness patients about what is permitted for use.
- Usually, whole blood, RBC, plt, plasma is not allowed
- Cell Saver, plasma proteins, clotting factors MAY be tolerated
- Knowing this, limit phlebotomy and still get Type and Screen x TWO
- Cohort study of JW surgical patients who refused RBC transfusions found 2.5x odds increase in mortality for every 1g/dL drop post-operatively. (1)
- Ethical concerns about patients refusing blood products when altered. (2)
- Biblical basis:
- Genesis 9:3-5: “But you must not eat blood that has its lifeblood still in it.”
- Leviticus 17: “You must not eat the blood of any creature, because the life of every creature is its blood; anyone who eats it must be cut off.”
- Biblical basis:
Areas of Improvement
- Communication: There was no inter-facility hand-off done between hospitals. Patient arrived without records of procedure, name of surgeon and a poor understanding of his own medical history. ED team spent valuable time getting surgical history from outside hospital.
- Improper Triage: Patient triaged to level 3 despite being hypotensive and complaining of weakness.
- Cognitive Bias: MD was anchored to the recent surgical procedure as source of blood loss leading to premature closure of other causes of hypotension and anemia.
- Rule-Based Issues: Patient only had single IV placed and single Type and Screen sent. Patient was hypotensive, supra-therapeutic and anemic…with presumed bleeding. Rule is generally that 2 IVs and 2 Type and Screens should be placed and sent on hypotensive/bleeding patients.
References
- Tobian AA, Ness PM, Novick H, Carson PL. Time course and etiology of death in patients with severe anemia.Transfusion, Jul2009 Part 1 of 2, Vol. 49 Issue 7, p1395-1399, 5p, p1397.
- Megan L. Panico, Grace Y. Jenq, and Ursula C. Brewster. When a Patient Refuses Life-Saving Care: Issues Raised When Treating a Jehovah’s Witness. American Journal of Kidney Diseases, 2011-10-01, Volume 58, Issue 4, Pages 647-653.





