
Author: Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital)
You receive a radio call from an EMS unit. They are transporting a 61-year-old male who collapsed approximately 5 minutes ago. He is currently in ventricular fibrillation, and the EMS crew is actively doing compressions. They have obtained IV access, defibrillated the patient once, given 1mg epinephrine IV, and are actively bagging the patient. The patient arrives, and you take over the resuscitation. Your partner cleanly intubates the patient while chest compressions are ongoing. The patient receives another defibrillation, and compressions resume. Should the patient receive more epinephrine? What’s the evidence behind its use?
Sudden cardiac arrest accounts for over 450,000 deaths per year in the U.S., with 15% of total deaths due to arrest.1-4 Close to half are out-of-hospital, with poor survival rate (7-9%).1-5
A prior emdocs.net post evaluated epinephrine use in cardiac arrest. Please see this at: http://www.emdocs.net/epinephrine-cardiac-arrest/. Epinephrine is a staple of the AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Updated guidelines were released in 2015, building on a “Chain of Survival”: recognition and activation of emergency response system, immediate high-quality cardiopulmonary resuscitation (CPR), rapid defibrillation, basic and advanced emergency medical services, and advanced life support and post arrest care including advanced cardiac life support (ACLS) for out-of-hospital cardiac arrest (OHCA).7,8 ACLS is considered the standard of care in cardiac arrest, though some argue a lack of evidence.
For more information on the updated guidelines, see http://eccguidelines.heart.org/wp-content/uploads/2015/10/2015-AHA-Guidelines-Highlights-English.pdf, https://emergencymedicinecases.com/acls-guidelines-2015-cardiac-arrest/, https://first10em.com/2015/10/21/acls-2015/, http://rebelem.com/rebel-cast-wee-our-top-5-aha-2015-guideline-updates-for-cpr-and-ecc/.
The Myth: Epinephrine improves patient survival and neurologic outcome in cardiac arrest.
Is this important?
A class IIb recommendation from the AHA states “standard dose epinephrine may be reasonable for patients with cardiac arrest” in the 2015 updates, with doses of 1mg of 1:10,000 epinephrine every 3-5 minutes intravenously.7 Epinephrine has alpha and beta adrenergic effects, which are thought to improve coronary perfusion pressure, though the effect on cerebral perfusion is controversial (and may worsen cerebral perfusion).
The recommendation for epinephrine is based on studies in the 1960s, which found epinephrine given to asphyxiated dogs improved survival.9 The alpha-adrenergic effects improved coronary perfusion in these dogs, with some benefit in survival.
If some is good, is more better? High dose epinephrine was assumed to be better, with several studies finding increased ROSC and survival to hospital admission, but no improvement in survival to hospital discharge or neurologic recovery.10-14 Studies suggest worse survival to hospital discharge and neurologic recovery with higher doses of epinephrine.7,15-20
What about standard dose epinephrine? Studies suggest improvement in ROSC, but worse neurologic and survival to discharge. Why? The beta agonism provided by epinephrine increases myocardial work, increases tachydysrhythmias, promotes thrombogenesis and platelet activation, and reduces microvascular perfusion (including the brain).7,15
Now down to the nuts and bolts: the evidence on epinephrine…
Table 1 shows the studies on epinephrine. A study in 2011 evaluated over 600 patients with OHCA (one of the few randomized trials).16 Improved likelihood of ROSC, 24% in the epinephrine group versus 8%, with an odds ratio (OR) of 3.4 (95% CI 2.0-5.6) was found. Patients demonstrated no improvement in survival to hospital discharge.16 Ong et al. in 2007 found no difference in survival to discharge, survival to admission, or ROSC with epinephrine versus no epinephrine.17
Nakahara et al. conducted a retrospective study comparing epinephrine versus no epinephrine for patients with ventricular fibrillation, PEA, or asystole.18 Higher overall survival with epinephrine (17.0% vs 13.4%) was found, but not neurologically intact survival.18 Hagihara et al. conducted a prospective non-randomized analysis of over 400,000 patients and found an increase in ROSC with epinephrine (adjusted odds ratio 2.36), but no increase in survival or functional outcome.19 As discussed, ROSC occurred in the epinephrine group at higher rate (18.5% vs. 5.7%), but patients receiving epinephrine had lower survival at one month and worse neurologic outcome.19
One study found those with initially shockable rhythm demonstrated worse outcomes if they receive epinephrine for prehospital ROSC, survival at one month, and neurologic outcome at one month.20 A Swedish study found patients receiving epinephrine experience lower survival, with OR 0.30 (95% CI 0.07-0.82).21
How about BLS compared with ACLS?
ACLS measures include epinephrine, as compared with BLS focusing on optimizing compressions. Stiell et al. in 2004 analyzed 1,400 patients before use of ACLS measures, followed by 4,300 patients after ACLS was implemented.22 Admission rate increased by 3.7% (10.9% to 14.6%), but survival to discharge did not change. Survivor neurologic status worsened after ACLS implementation (78.3% versus 66.8%).22 Olasveengen et al. evaluated ACLS with and without epinephrine, finding a 40% rate of ROSC in the group receiving epinephrine, versus 25% in the group receiving no epinephrine.23 Survival to discharge and neurologic outcomes were similar, though the epinephrine group had higher hospital admission rates.23 Sanghavi et al. compared BLS and ACLS in an observational cohort study.24 BLS patients had higher survival to hospital discharge (13.1% versus 9.2%), improved survival to 90 days, and better neurologic function.24
Table 1 – Studies evaluating epinephrine16-24

The Bottom Line: Epinephrine can increase ROSC, but it does not improve survival to hospital discharge or neurological improvement and may worsen these outcomes.
How does this change practice? Epinephrine is a significant component of the AHA guidelines, despite the controversial literature. A role may exist for epinephrine, though further study is required. Studies suggest three phases (electrical, circulatory, and metabolic) are present in cardiac arrest.25 The electrical phase needs rapid defibrillation and compressions.15,25 The circulatory phase (within 10 minutes of arrest) focuses on perfusion, where epinephrine may improve cardiac perfusion. Epinephrine during the final metabolic phase (greater than 10 minutes after arrest) can impair oxygen utilization, increase oxygen demand and ischemia, cause dysrhythmia, increase clotting, and increase lactate.15,25
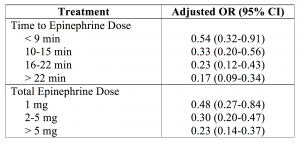
The timing and total dose of epinephrine can impact patient outcome.7,15,25-27 A study by Dumas et al. suggests timing of first administration and total epinephrine given impacts survival (with less epinephrine given related to improved outcome).25 This study found that 17% of patients in the group receiving epinephrine demonstrated a good outcome defined by “favorable discharge outcome coded by Cerebral Performance Category,” compared to 63% not receiving epinephrine. However, in this study patients with a shockable rhythm, patients receiving 1mg epinephrine, and patients receiving epinephrine less than 9 minutes after arrest demonstrate the best outcomes, not impacted by the total time of resuscitation. Patients receiving late or multiple doses of epinephrine have decreased neurologic survival.25
Table 2 – Epinephrine Dosing Outcomes25
Epinephrine within 10 minutes of arrest may provide the most benefit. Koscik et al. found earlier provision of epinephrine improved ROSC, from 21.5% to 48.6% (OR 3.45).26 Nakahara et al. compared early epinephrine in OHCA (within 10 minutes of arrest), finding early epinephrine was associated with survival (OR 1.73, 95% CI 1.46-2.04) and improved neurologic outcome (OR 1.39, 95% CI 1.08-1.78).27 However, there is potential harm with epinephrine within the first two minutes of arrest.27 Anderson et al. compared epinephrine before or after the second defibrillation attempt.28 Patients receiving epinephrine before the second defibrillation demonstrated decreased survival (OR 0.70), decreased functional outcome (OR 0.69), and decreased ROSC (OR 0.71). This study suggests epinephrine within the first two minutes after arrest can be harmful, and they recommend epinephrine should be given after the second defibrillation.27
Some support targeting coronary perfusion pressure (CPP), or the aortic to right atrial pressure gradient during the relaxation phase of CPR. Targeting coronary perfusion pressure is supported by several animal studies.29,30 CPP levels > 15 mm Hg demonstrate greater likelihood of ROSC.31 Epinephrine is most commonly used to maintain CPP levels with compressions. However, this needs further study and requires the use of invasive monitoring.25,31
What improves outcomes?
Components that improve outcomes include witnessed arrest, witnessed by EMS, bystander CPR, shockable rhythm (VF/VT), early defibrillation, minimal interruptions to CPR, automated external AED use, and therapeutic hypothermia in comatose cardiac arrest patients.7,15,32 Optimal chest compressions and early defibrillation if warranted are essential.7 Emergency PCI is recommended for all patients with STEMI and for hemodynamically unstable patients without ST elevation infarction if a cardiovascular lesion is suspected. Targeted temperature management between 32oC and 36oC is acceptable for comatose patients with ROSC.7 The 2015 recommendations for BLS measures are shown below. 7,32

Bottom Line: The most important aspect of care in cardiac arrest is basic life support measures with compressions and early defibrillation.
Takeaways:
– 2015 AHA Guidelines state epinephrine is reasonable to give for patients in cardiac arrest.
– Recommendations are based on studies with asphyxiated dogs in the 1960s.
– High dose epinephrine is harmful and is not advised.
– Epinephrine can increase ROSC, but it may worsen neurologic outcome and survival upon discharge.
– Epinephrine may provide the greatest benefit if given within 10 minutes of arrest (though it may be harmful if given before 2 minutes).
– BLS measures with optimal compressions and early defibrillation are essential!
References / Further Reading
- Zheng ZJ, Croft JB, Giles WH, Mensah GA. Sudden cardiac death in the United States, 1989 to 1998. Circulation 2001; 104:2158.
- Rea TD, Pearce RM, Raghunathan TE, et al. Incidence of out-of-hospital cardiac arrest. Am J Cardiol 2004; 93:1455.
- Centers for Disease Control and Prevention (CDC). State-specific mortality from sudden cardiac death–United States, 1999. MMWR Morb Mortal Wkly Rep 2002; 51:123.
- Chugh SS, Jui J, Gunson K, et al. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardio 2004;44:1268.
- Kuller LH. Sudden death–definition and epidemiologic considerations. Prog Cardiovasc Dis 1980; 23:1.
- Gillum RF. Sudden coronary death in the United States: 1980-1985. Circulation 1989; 79:756.
- Link MS, Berkow LC, Kudenchuk PJ, et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132:S444-S464.
- Neumar RW, Otto CW, Link MS, et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010;122(Suppl 3):S729-67.
- Callaham M. Evidence in support of a back-to-basics approach in out-of-hospital cardiopulmonary resuscitation vs. “advanced treatment.” JAMA Intern Med. 2015;175:205-206.
- Stiell IG, Hebert PC, Weitzman BN, et al. High-dose epinephrine in adult cardiac arrest. N Engl J Med. 1992;327:1045-1050.
- Brown CG, Martin DR, Pepe PE, et al. A comparison of standard-dose and high-dose epinephrine in cardiac arrest outside the hospital. The Multicenter High-Dose Epinephrine Study Group. N Engl J Med. 1992;327:1051-1055.
- Rivers EP, Wortsman J, Rady MY, et al. The effect of total cumulative epinephrine dose administered during human CPR on hemodynamic, oxygen transport, and utilization variables in the postresuscitation period. Chest. 1994;106:1499-1507.
- Behringer W, Kittler H, Sterz F, et al. Cumulative epinephrine dose during cardiopulmonary resuscitation and neurologic outcome. Ann Intern Med. 1998;129:450-456.
- Guegniaud PY, Mols P, Goldstein P, et al. A comparison of repeated high doses and repeated standard doses of epinephrine for cardiac arrest outside the hospital. N Engl J Med. 1998;339:1595-1601.
- Callaway CW. Questioning the use of epinephrine to treat cardiac arrest. JAMA. 2012;307:1198-1199.
- Jacobs IG, Finn JC, Jelinek GA, Oxer HF, Thompson PL. Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind placebo-controlled trial. Resuscitation. 2011 Sep;82(9):1138-43.
- Ong ME, Tan EH, Ng FS, Panchalingham A, Lim SH, Manning PG, et al. Survival outcomes with the introduction of intravenous epinephrine in the management of out-of-hospital cardiac arrest. Ann Emerg Med. 2007 Dec;50(6):635-42.
- Nakahara S, Tomio J, Takahashi H, et al. Evaluation of pre-hospital administration of adrenaline (epinephrine) by emergency medical services for patients with out of hospital cardiac arrest in Japan: controlled propensity matched retrospective cohort study. The BMJ. 2013;347:f6829. doi:10.1136/bmj.f6829.
- Hagihara A, Hasegawa M, Abe T, Nagata T, Wakata Y, Miyazaki S. Prehospital epinephrine use and survival among patients with out-of-hospital cardiac arrest. JAMA. 2012 Mar 21;307(11):1161-8. doi: 10.1001/jama.2012.294.
- Goto Y, Maeda T, Goto YN. Effects of prehospital epinephrine during out-of-hospital cardiac arrest with initial non-shockable rhythm: an observational cohort study. Critical Care. 2013;17(5):R188. doi:10.1186/cc12872.
- Holmberg M, Holmberg S, Herlitz J. Low chance of survival among patients requiring adrenaline (epinephrine) or intubation after out-of-hospital cardiac arrest in Sweden. Resuscitation. 2002 Jul;54(1):37-45.
- Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M; Ontario Prehospital Advanced Life Support Study Group. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004 Aug 12;351(7):647-56.
- Olasveengen TM, Sunde K, Brunborg C, Thowsen J, Steen PA, Wik L. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA. 2009 Nov 25;302(20):2222-9.
- Sanghavi P, Jena AB, Newhouse JP, Zaslavsky AM. Outcomes After Out-of-Hospital Cardiac Arrest Treated by Basic vs Advanced Life Support. JAMA Intern Med 2015;175(2):196-204.
- Dumas F, Bougouin W, Geri G, Lamhaut L, Bougle A, Daviaud F, et al. Is epinephrine during cardiac arrest associated with worse outcomes in resuscitated patients? J Am Coll Cardiol. 2014; 64(22):2360–7.
- Koscik C, Pinawin A, McGovern H, Allen D, Media DE, Ferguson T, Hopkins W, Sawyer KN, Boura J, Swor R. Rapid epinephrine administration improves early outcomes in out-of-hospital cardiac arrest. Resuscitation. 2013 Jul;84(7):915-20.
- Nakahara S, Tomio J, Nishida M, Morimura N, Ichikawa M, Sakamoto T. Association between timing of epinephrine administration and intact neurologic survival following out-of-hospital cardiac arrest in Japan: a population-based prospective observational study. Acad Emerg Med. 2012 Jul;19(7):782-92.
- Andersen LW, Kurth T, Chase M, et al. Early administration of epinephrine (adrenaline) in patients with cardiac arrest with initial shockable rhythm in hospital: propensity score matched analysis. BMJ 2016; 353:i1577.
- Friess SH, Sutton RM, French B, et al. Hemodynamic Directed CPR Improves Cerebral Perfusion Pressure and Brain Tissue Oxygenation. Resuscitation. 2014;85(9):1298-1303.
- Sutton RM, Friess SH, Naim MY, et al. Patient-centric Blood Pressure–targeted Cardiopulmonary Resuscitation Improves Survival from Cardiac Arrest. American Journal of Respiratory and Critical Care Medicine. 2014;190(11):1255-1262.
- Paradis NA, Martin GB, Rivers EP, et al. Coronary Perfusion Pressure and the Return of Spontaneous Circulation in Human Cardiopulmonary Resuscitation. JAMA. 1990;263(8):1106-1113.
- Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010 Jan;3(1):63-81.







5 thoughts on “A Myth Revisited: Epinephrine for Cardiac Arrest”
[…] la lectura de este articulo, revisando el mito de la epinefrina en el paro cardíaco. Se reafirma que lo más importante sigue […]
Pingback: Episode 96 Beyond ACLS Cardiac Arrest - Live from EMU Conference 2017 - Emergency Medicine Cases
Pingback: emDOCs.net – Emergency Medicine EducationJournalFeed Weekly Wrap-Up - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationJournalFeed Weekly Wrap-Up - emDOCs.net - Emergency Medicine Education
Pingback: Two Common EM Myths Demystified – JournalFeed