Welcome back to Small Talk. Every first Wednesday of the month we will release high yield PEM content written by PEM talent from around the country. We hope you enjoy these reviews. Comments, questions, accolades or concerns: feel free to reach out to Joe Ravera, MD (pemgemspod@gmail.com).
Author: Andrew Meshnick, MD (Pediatric Resident, University of Vermont Children’s Hospital); Joseph Ravera MD (@pemuvm1, Director of Pediatric Emergency Medicine, Assistant Professor of Emergency Medicine, University of Vermont Medical Center) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case:
A 9-year-old is referred to the ED from the pediatrician for weight loss, abdominal pain, and increased fatigue. She has stable vital signs and on exam does appear fatigued but nontoxic. She is ambulatory, and within the limits of a busy emergency department hallway bed, has an unremarkable exam. A CBC, CMP, and an abdominal ultrasound are ordered from tirage: they show elevated transaminases, intraabdominal free fluid, and a thickened gallbladder wall without evidence of gallstones.
A 20cc/kg bolus is about to start when a cardiac POCUS is performed.
The POCUS shows poor ventricular contraction. The bolus is cancelled, and orders are placed for EKG, chest X-ray, troponin, and BNP.
Demographics of Congestive Heart Failure in Children:
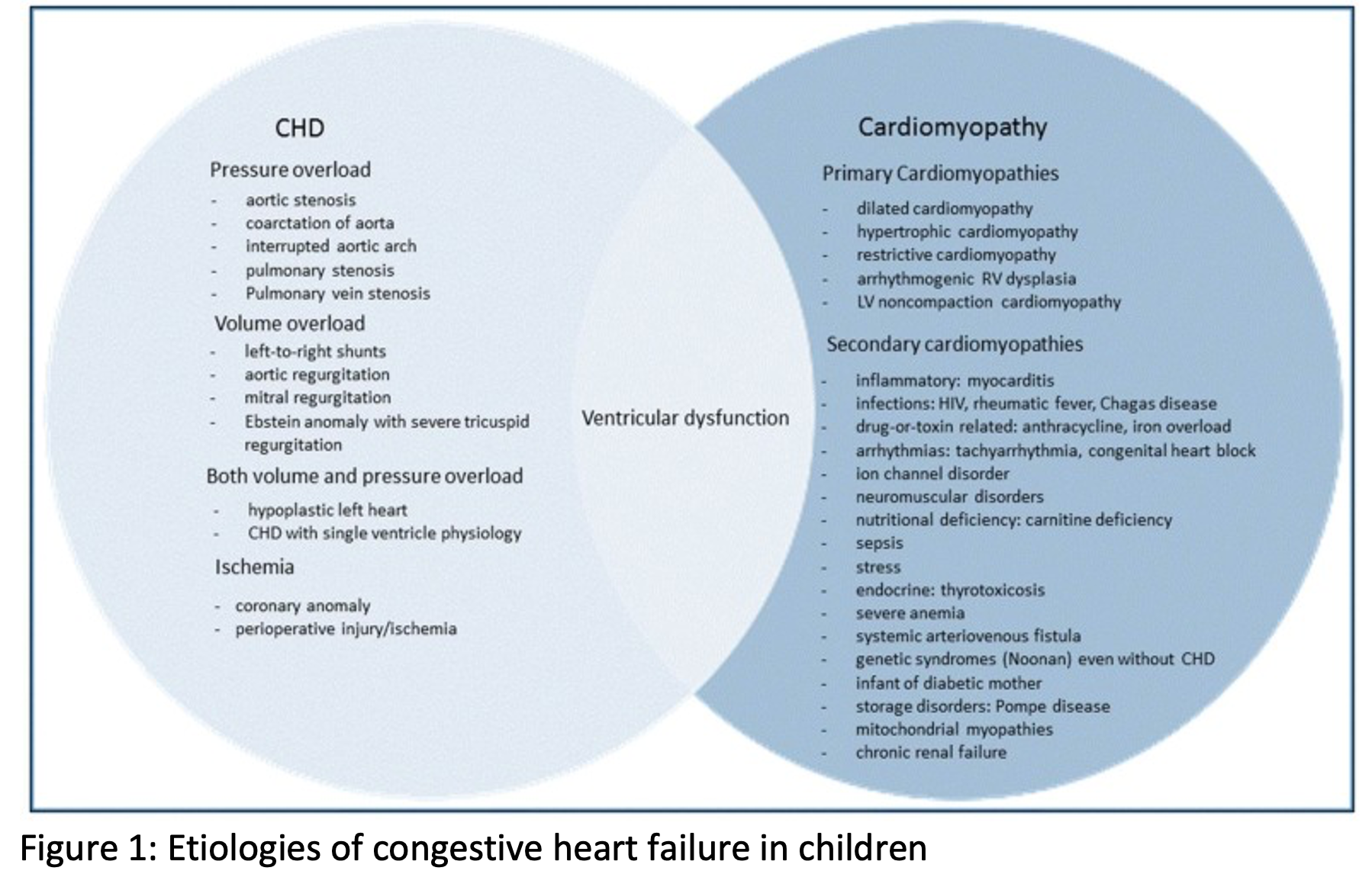
Congestive heart failure is defined as a clinical syndrome when cardiac output is insufficient to meet the metabolic demands of the body.[1] Heart failure in children may be classified as syndromes of excessive preload, excessive afterload, arrhythmia, or decreased contractility (cardiomyopathy).[2]
Pediatric heart failure is rare with an estimated prevalence between 1 and 7 per 100,000 in the United States and a worldwide presence ranging as high as 83/100,000 in some areas.[1] The most common cause of pediatric heart failure in the United States is underlying congenital heart disease. Given the widespread availability of diagnostic testing, a large percentage of these children will present with a known structural lesion and already be followed closely by a cardiologist. If these children present to the ED, early consultation with pediatric cardiologyis encouraged. In the absence of known congenital heart disease, a child with congestive heart failure almost always has a cardiomyopathy (often dilated), which is defined as cardiac muscle dysfunction. Multiple distinct disease processes may result in the development of cardiomyopathy.[1,2]
The Challenge of Recognizing an Underlying Etiology
The difficult part for an emergency physician is that we must be aware that children without a congenital heart disease may develop heart failure, and it’s these children who can have severe consequences. While cardiomyopathy is sometimes a treatable condition, if missed it can progress to more fulminant cardiomyopathy and congestive heart failure. Etiologies include:
Inflammatory Conditions – Kawasaki Disease and MIS-C: EM clinicians must have a high index of suspicion for these conditions, particularly in cases of prolonged fever. It should also be noted that infants often present with atypical or incomplete Kawasaki disease, and prolonged fever without a clear etiology should raise the suspicion even in the absence of other features. When in doubt, consider obtaining several laboratory tests and consulting your inpatient pediatrics service for fever lasting greater than 5 days. More information on this can be found in a previous EMdocs post.
Covid-19 Associated Myocarditis: While there is a small risk associated Covid-19 vaccination, the risk is 6 to 34 times higher in children infected with Covid-19 who have not received an mRNA vaccine.[3] Children with post vaccination myocarditis tend to be adolescents, and they present with chest pain, shortness of breath, and/or persistent tachycardia. Only a small minority of patients with post vaccination myocarditis developed a long-standing cardiomyopathy.
Tachycardia Mediated Cardiomyopathy: Infants with structurally normal hearts often tolerate dysrhythmia quite well. Up to 50% of cases of infant SVT are clinically silent. In these cases, prolonged tachycardia (days to months) can lead to a tachycardia mediated cardiomyopathy (Figure 2 and 3). More information about pediatric dysrhythmia can be found in a previous EMdocs post.
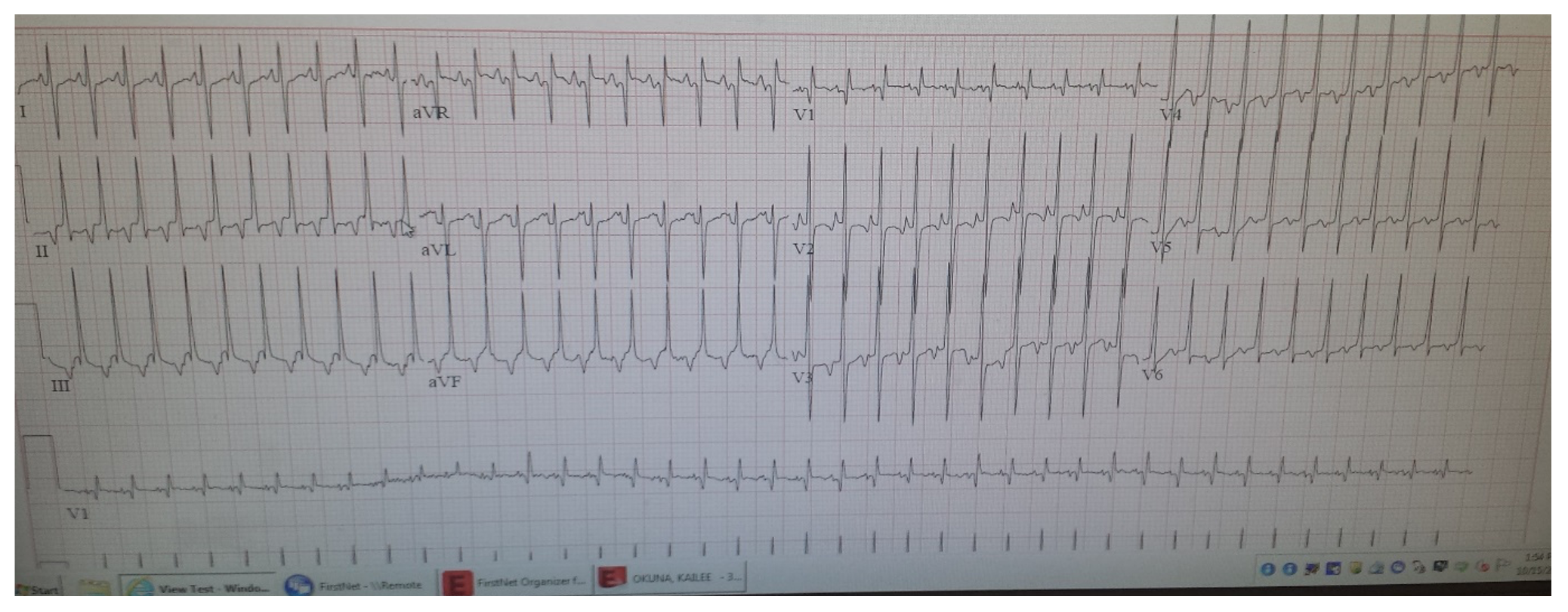

Figure 2 & 3: Persistent SVT leading to cardiomyopathy and tachycardia mediated cardiomyopathy in a 5-month-old.
Infectious Myocarditis: Coxsackie B and Adenovirus are documented causes of viral myocarditis, but several other viruses have been implicated.[4] The initial presentation of viral myocarditis can be difficult if not impossible to differentiate from the thousands of viral syndromes that we see. Persistent tachycardia in the absence of fever, pain, or anxiety is a possible clinical clue that should raise your suspicion of myocarditis. If suspected, we recommend an evaluation with laboratory markers including troponin and BNP, with consideration of admission for further diagnostic tests such as an echocardiogram or cardiac MRI. Bedside US can assist. Although rare in the United States, Chagas disease and rheumatic heart disease are known causes of cardiomyopathy with a larger burden of disease worldwide. If there is a concerning travel history or a patient from an endemic area, consideration should be given to these diagnoses.
Given that are multiple etiologies that potentially lead to cardiomyopathy, there is not a “standard work up” or recommended tests. However, as stated, the challenge for EM physicians is to recognize the possible conditions that may lead to cardiomyopathy and direct their work up accordingly.
The End Stage: Recognition and Management of Congestive Heart Failure and Dilated Cardiomyopathy
Adult congestive heart failure is typically recognizable by the clinical signs of orthopnea, weight gain, paroxysmal nocturnal dyspnea (PND), and pedal edema. However, children often present differently. Infants with heart failure can present with failure to gain weight, poor feeding, increased fatigue, and tachypnea. Peripheral edema is rare in pediatric patients with heart failure. Hepatomegaly with an increased liver edge is a sign of hepatic congestion, and thus palpation for the liver edge is recommended in suspected cases. Older children with heart failure may present with exercise intolerance, decreased energy, anorexia, cough, or crackles. At its most extreme, children can also present with fulminant cardiac failure and cardiac arrest.
Although the presentation is limited there can be several clinical clues. Abdominal pathology such as a transaminitis or ascites in the absences of demonstrable abdominal pathology should raise your suspicion. Additionally, a child who has a respiratory decompensation during or following the administration of IV fluids should raise the suspicion for cardiomyopathy.
Diagnostic Studies in the Emergency Department
If suspected, there are several tests available for the diagnosis of cardiomyopathy:
– Point of Care Ultrasound: Although specific measurements of EF are outside the scope for most EM clinicians, a quick cardiac POCUS can give a ballpark idea of contractility, the presence of cardiac effusion, and pulmonary edema.
– Chest X-Ray: This test can evaluate for cardiomegaly and pulmonary vascular congestion. A normal pediatric heart should be no more than 50% of the diameter of the chest.
– Electrocardiogram: This can evaluate for ischemia and arrhythmia.
– Laboratory Assessment: BNP and troponin can assist. ESR and CRP can assess for inflammation. Elevations in LFTs may also be suggestive of hepatic congestion secondary to right heart failure. Electrolytes should be assessed for derangement, and renal function should also be assessed.
Treatment And Disposition
Once a cardiomyopathy and congestive heart failure are recognized, prompt consultation with a pediatric cardiologist and PICU is recommended. These children can be extremely medically fragile and may decompensate quickly. While preparing for admission or transfer, emergency department management should focus on the following areas:
– Optimize volume status: These children often present volume overladed and despite soft blood pressures, do not need further volume. If there is a need to give volume it should be done in small boluses (i.e., 5 cc/kg) with close monitoring and cessation of fluids if they begin to decompensate. Consider diuretics such as furosemide 1mg/kg IV at the direction of pediatric cardiology or PICU.
– Ionotropic support: If children are both volume overloaded and hypotensive or progressing to fulminant cardiac failure ,inotropic support will be needed. Ideally this is done with the help of specialty consultation, but epinephrine or norepinephrine (0.05mcg/kg/min) infusion should be considered first line. Providers can consider further addition of milrinone (intial loading dose of 50mcg/kg, followed by 0.25-0.75mcg/kg/min) or dobutamine to improve contractility.
– Aggressive arrythmia treatment: Unlike a healthy heart, these children will not tolerate arrhythmias and may rapidly decompensate. To make matters worse the underlying cardiomyopathy is a set up for arrythmias. Initial efforts should be aimed at correcting any electrolyte abnormalities as these can cuase further arrhythmias. If there is persistent ventricular ectopy or short runs of a ventricular arrythmia, an antiarrhythmic should be considered. While consultation for correct medication choice is ideal, we recommend a lidocaine infusion (1mg/kg, followed by 20mcg/kg/min) as first line for ventricular ectopy. For sustained arrythmias, have a low threshold for electrical cardioversion.
Pearls and Pitfalls
- Congenital heart disease is the most common cause of CHF in the Untied States, and early consultation with a pediatric cardiologist for kids with known structural lesions can assist with evaluation and management.
- EM clinicians need to maintain an index of suspicion for multiple etiologies that can progress to a cardiomyopathy.
- Consider a POCUS as a quick screening test.
- Fatigue, weight loss, vomiting, and abdominal ascites may be the first presentation of cardiomyopathy.
- Decompensation with fluids are concerning for cardiomyopathy.
- Once recognized, these children should be transferred to tertiary/quaternary centers ASAP
- Aggressively treat all arrhythmias in these children.
Case Conclusion
The chest X-ray was consistent with cardiomegaly, the troponin was positive at 0.2, and the BNP was 6000. The EKG had low voltages but was otherwise unremarkable.
The child was admitted to the PICU, pediatric cardiology was consulted, and the child’s echocardiogram demonstrated dilated cardiomyopathy and an EF of 10-15%. She was started on furosemide and a milrinone drip. She was transferred to a quaternary center the following day.
References
- Das BB. Current State of Pediatric Heart Failure. Children (Basel). 2018;5(7):88. Published 2018 Jun 28. doi:10.3390/children5070088
- Madriago E, Silberbach M. Heart failure in infants and children. Pediatr Rev. 2010 Jan;31(1):4-12. doi: 10.1542/pir.31-1-4. Erratum in: Pediatr Rev. 2010 Apr;31(4):158. PMID: 20048034.
- https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-08-30/06-COVID-Rosenblum-508.pdf
- Law YM, Lal AK, Chen S, Čiháková D, Cooper LT Jr, Deshpande S, Godown J, Grosse-Wortmann L, Robinson JD, Towbin JA; American Heart Association Pediatric Heart Failure and Transplantation Committee of the Council on Lifelong Congenital Heart Disease and Heart Health in the Young and Stroke Council. Diagnosis and Management of Myocarditis in Children: A Scientific Statement From the American Heart Association. Circulation. 2021 Aug 10;144(6):e123-e135. doi: 10.1161/CIR.0000000000001001. Epub 2021 Jul 7. Erratum in: Circulation. 2021 Aug 10;144(6):e149. PMID: 34229446.






