Welcome back to Small Talk; a new monthly section from emDOCs. Every first Wednesday of the month we will release high yield PEM content written by PEM talent from around the country. We hope you enjoy these reviews. Comments, questions, accolades or concerns: feel free to reach out to Joe Ravera, MD (pemgemspod@gmail.com).
Authors: Laura Le, MD (PGY 2, Department of Emergency Medicine, Dartmouth-Hitchcock Medical Center); Joe Ravera, MD (@pemuvm1, Director of Pediatric Emergency Medicine, Assistant Professor of Surgery, Division of Emergency Medicine, University of Vermont Medical Center) // Reviewed by Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 22-month-old female comes in the Emergency Department with concern for a seizure. The mother states that she witnessed the child fall forward and have a tonic-clonic seizure for approximately 1 minute. She was confused after for approximately 15 to 20 minutes with no focal deficits. Mother states over the past 3 days, the child has had vomiting and decreased PO intake but no diarrhea noted. She was noted to be somewhat flushed on arrival.
Exam
Vital signs: BP 89/74, Temp 36.7 C (99 F) rectally, HR 117, RR 22, SpO2 99%, Fingerstick 54 mg/dL
General: sleepy child laying in mother’s arms but arousable to voice. Cheeks are somewhat flushed with dry mucous membranes.
Abdomen: no abdominal tenderness, no hepatosplenomegaly.
Neuro: no focal neurological deficits, moves all extremities and is able to ambulate around the room without issue.
Skin: no obvious rashes or pigmentation to skin, capillary refill > 3 seconds.
Clinical Presentation and Diagnosis
Hypoglycemia has a spectrum of presentations from jitteriness and agitation to the more severe altered mental status, seizures and obtundation.1,2 With the ubiquitous nature of point of care glucose machines and a low threshold to test, it is rare to miss the diagnosis. In these authors experience, the reliance on EMS to check glucose can sometimes lead to a delay when a child who presents as a walk in.
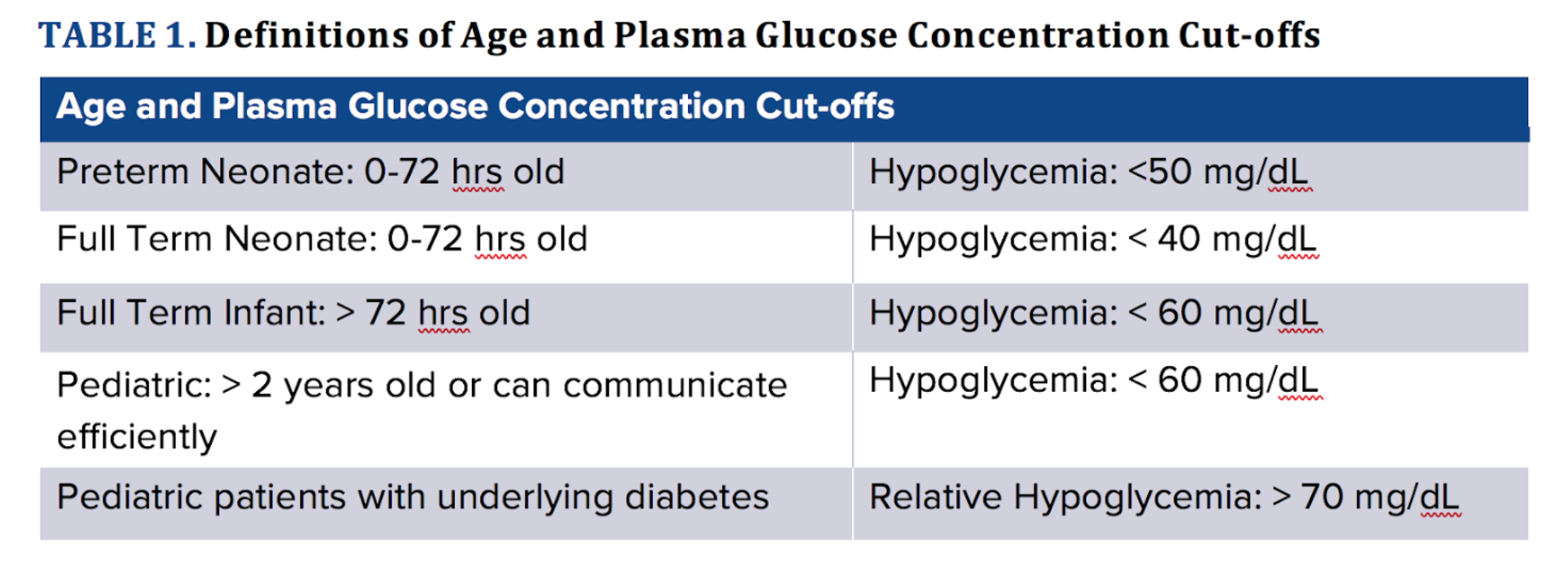
Normal blood sugar can vary with age and presence or absence of diabetes. There are certain cut-offs given age ranges and it can be relative hypoglycemia if a patient has poorly controlled diabetes. Roughly, however, hypoglycemia is based on age and is delineated in the chart below. For our patient, given that she was symptomatic with a documented low blood sugar, she fits the criteria (Table 1).
Etiology of Hypoglycemia
Pediatric hypoglycemia often presents in the context of an illness and decreased oral intake. While this can be the sole cause this is typically with severe dehydration and a prolonged period without PO. In addition, critical illness, such as sepsis, can produce hypoglycemia, but this is typically with more advanced presentations. In cases of rapid onset, it is important to remember that an illness can exacerbate a known or unmask and unknown inborn error of metabolism.3,4
In the absence of an illness or other obvious clinical cause other etiologies can be stratified by age:
For infants consider a hormone deficiency or dysregulation of glucose metabolism:
- A hormone deficiency (e.g. Congenital adrenal hyperplasia, hypopituitarism, growth hormone or cortisol deficiency)
- An inborn error of metabolism of glucose or glycogen (e.g. glycogen storage disease)
For toddlers consider an ingestion or dysregulation of lipid metabolism:
- Accidental ingestion of an oral hypoglycemic (note that the presentation can be delayed and have lasting effects, particularly with sulfonylurea ingestion)5,6
- Fatty acid oxidation defect (particularly if non ketotic hypoglycemia)
For older children consider an autoimmune or toxicologic cause:
- Central nervous system mass
- Addison’s disease
- Intentional or accidental toxic ingestion such as alcohol or medications
- Exogenous insulin use if known diabetic
Emergency Department Evaluation and Work Up
When evaluating a patient, physical exam, collateral, and history are important to determining etiology. As result, history taking is essential and can often elucidate the etiology – consider asking about birth weight, family history of disease, family medications at home, environment and risk for possible ingestion, hyperpigmentation, new foods, or recent steroid use.
If there is an obvious clinical answer, such as poor PO intake or exogenous insulin use, a child with ketotic hypoglycemia can treated symptomatically and often observed for a set period of time without further work up.
In the absence of a clinical answer or if there is non-ketotic hypoglycemia consider an expanded work up:
- insulin level/c-peptide
- cortisol
- growth hormone
- lactate
- ammonia
- free fatty acids
If you suspect an inborn error of metabolism, consider getting amino acids, carnitine, acylcarnitine, urine organic acids.
If you suspect possible toxic ingestion, consider toxicology screen for ingestion such as ethanol, salicylates, beta-blockers, oral hypoglycemics.
In complex cases the interpretation of the bicarbonate, ketones, lactate and free fatty acids can provide a clue to the diagnosis. (Figure 1)

Treatment
To manage hypoglycemia, you must make sure the patient is actually hypoglycemic. Oftentimes, fingerstick glucometers can be inaccurate and you must confirm with venous blood sample. Once confirmed, you can initiate treatment.7
If the patient is awake and alert, you can consider giving oral glucose in the form of juice, popsicles, frosting, etc.
If the patient is unable to take PO due to altered mental status, active seizure, or inability to maintain airway, administer parenteral replacement with IV dextrose.
If the patient is a known diabetic, consider IM glucagon (0.5 mg if <25kg and 1mg if >25kg) to assist with hypoglycemia.
You can use the memory aid of the “rule of 50” or the “5/2/1 rule” – the concentration of dextrose and the volume per kilogram should equal 50. Of note, oftentimes D50 is avoided given its hypertonicity and should not be given through a peripheral IV.

Key: When you multiple the two values together, they all equal 50 (for example, 25 x 2mL/kg = 50)
Sugars should be rechecked approximately 15 minutes after initial dextrose supplementation. If the patient has persistent hypoglycemia, consider another bolus and initiating maintenance fluids with D10NS at 1.5x maintenance rate.
Disposition
If the cause of hypoglycemia is known or clear-cut with a reassuring history, physical exam and overall clinical picture, short term observation with blood sugar checks and discharge is reasonable. However, if the story is unclear or there are abnormal findings to suggest ingestion, infection, or metabolic issue, consider inpatient admission for close observation and further work-up.
Case Conclusion
The patient was noted to have an elevated beta-hydroxybutyrate and the remainder of her hypoglycemic work-up was negative. Working diagnosis noted to be ketotic hypoglycemia and she was told to follow-up outpatient with endocrinology. No further episodes of hypoglycemia were documented during the patient’s inpatient stay with reassuring labs.
Pearls
- Confirm POC check with a plasma.
- Get labs/urine with multiple tubes so that other labs can be added.
- Supplement with oral if they tolerate PO.
- Supplement with IV using D10/D25/D50 at a rate of 5/2/1 mL/kg if they cannot tolerate PO.
- After bolus, POC check after 15 minutes.
- Consider inpatient admission if refractory to bolus or suspicion for other cause.
References:
- Ahmed FW, Majeed MS, Kirresh O. Non-diabetic Hypoglycemia. [Updated 2021 Jul 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan- Available from: https://www.ncbi.nlm.nih.gov/books/NBK573079/
- Mathew P, Thoppil D. Hypoglycemia. [Updated 2021 Jan 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534841/
- Weinstein DA, Steuerwald U, De Souza CFM, Derks TGJ. Inborn Errors of Metabolism with Hypoglycemia: Glycogen Storage Diseases and Inherited Disorders of Gluconeogenesis. Pediatr Clin North Am. 2018 Apr;65(2):247-265. doi: 10.1016/j.pcl.2017.11.005. PMID: 29502912.
- Kaplowitz P, Sekizkardes H. Clinical and laboratory characteristics and follow up of 62 cases of ketotic hypoglycemia: a retrospective study. Int J Pediatr Endocrinol. 2019;2019:3. doi: 10.1186/s13633-019-0066-9. Epub 2019 Nov 2. PMID: 31700521; PMCID: PMC6825346.
- Calello, Diane & Kelly, Andrea & Osterhoudt, Kevin. (2006). Case files of the Medical Toxicology Fellowship Training Program at the Children’s Hospital of Philadelphia: a pediatric exploratory sulfonylurea ingestion. Journal of medical toxicology: official journal of the American College of Medical Toxicology. 2. 19-24. 10.1007/BF03161009.
- Lung DD, Olson KR. Hypoglycemia in pediatric sulfonylurea poisoning: an 8-year poison center retrospective study. Pediatrics. 2011 Jun;127(6):e1558-64. doi: 10.1542/peds.2010-3235. Epub 2011 May 23. PMID: 21606145.
- Thornton PS, Stanley CA, De Leon DD, Harris D, Haymond MW, Hussain K, Levitsky LL, Murad MH, Rozance PJ, Simmons RA, Sperling MA, Weinstein DA, White NH, Wolfsdorf JI; Pediatric Endocrine Society. Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children. J Pediatr. 2015 Aug;167(2):238-45. doi: 10.1016/j.jpeds.2015.03.057. Epub 2015 May 6. PMID: 25957977.




