Authors: Wes Trueblood, MD (Chief Resident at SAUSHEC, USAF) and Nick Weiss, DO (Chief Resident at SAUSHEC, USA) // Edited by Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
You’re working a busy shift when you see the local paramedics coming in with a 50-year-old female who called EMS for sudden onset of chest pain and shortness of breath. EMS reports she has been GCS 15 and hemodynamically stable except for an initial O2 sat of 89% and initial BP of 91/50. They established peripheral IV access and gave a fluid bolus with resulting improvement in the BP to 109/75, and her oxygenation is now 94% on 4L by nasal cannula. She is speaking short sentences and is mildly tachypneic but otherwise appears in no distress. You obtain an EKG which demonstrates sinus tachycardia with incomplete right bundle branch block, and order basic labs, troponin I, portable chest X-ray. The workup shows negative troponin, and CTPA demonstrates a large central PE with evidence of right ventricular dilation. Does this patient need systemic thrombolysis? In this review we will begin with the basics of PE diagnosis and treatment, then specifically attempt to address the question of which patients need systemic thrombolysis.
Background/Epidemiology
It is estimated that 600,000 PE’s occur yearly in the United States1,2. It is helpful to divide PE into the clinical categories of low-risk, submassive, and massive in the style of the American Heart Association. Low-risk patients are those without hemodynamic instability (normotensive) or evidence of right ventricular strain3. Submassive PE is defined as hemodynamic stability (normotensive) with evidence of right ventricular strain. Evidence of right ventricular strain includes RV dysfunction on bedside echo, RV dilation (RV:LV > 0.9), elevated BNP (>500 pg/mL), elevated troponin I or T (>0.4 ng/mL, >0.1 ng/mL respectively), new ECG changes (incomplete or complete RBBB, anteroseptal ST elevation or depression, anterolateral T wave inversion)3. Massive PE includes those patients with PE and hemodynamic instability. Hemodynamic instability is demonstrated by sustained hypotension (systolic blood pressure <90 mm Hg for at least 15 minutes or requiring inotropic support, not due to a cause other than PE, such as arrhythmia, hypovolemia, sepsis, or left ventricular dysfunction), pulselessness, or persistent profound bradycardia (heart rate <40 bpm with signs or symptoms of shock) 3. Hemodynamic instability has been found to occur in 4.2% of PE’s from the International Cooperative PE Registry, but this may reach as high as 22% in other series4,5.
The Role of the Emergency Physician
PE is strikingly common, but it can be missed. Massive PE in particular is often misdiagnosed as ACS or a primary unstable arrhythmia. The emergency physician can play a critical role in recognizing PE, resuscitating, and initiating potentially life-saving treatment.
Stabilizing the Patient
The evaluation of any ED patient begins with an assessment of the ABCs. In massive PE, patients can present in undifferentiated cardiopulmonary arrest. However, PE is a mercurial disease. Patients with similar risk factors, comorbidities, and clot burdens can present with wildly different clinical characteristics, from mildly symptomatic to cardiopulmonary arrest. It is critical, especially in the patient with massive PE, to establish airway stability, adequately oxygenate, and provide hemodynamic support in the form of measured intravenous fluids and vasopressors when needed6.
Historical Features
The hallmark of PE is dyspnea of any degree and pleuritic chest pain, although nearly one half of patients diagnosed with PE will report no chest pain7. According to the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) data the most often encountered symptoms associated with PE are; dyspnea at rest or with exertion (73%), pleuritic chest pain (66%), cough (37%) orthopnea (28%), calf or thigh pain and/or swelling (44%), wheezing (21%), hemoptysis (13%)8. Syncope as a presenting symptom of PE occurs in less than 10% of cases9.
Several clinical decision rules have been derived to determine pretest probability and help rule out the diagnosis of PE based on history and physical findings alone. A full discussion of these rules is beyond the scope of this review, however it is worth mentioning that the most commonly used rules are the Wells and PERC (Pulmonary Embolism Rule Out Criteria) scoring systems. The Wells clinical decision rule stratifies risk into low, moderate, and high-risk categories based on historical features and risk factors. There is a subjective component to the Wells scoring system which requires the clinician to determine whether an alternative diagnosis is more likely than PE. Additionally, d-dimer testing is utilized in patients categorized as low risk to exclude the diagnosis of PE without additional imaging10,11. The PERC rule was derived and externally validated for use in low risk patients. If negative, PE likelihood is <2%, thus requiring no further testing12,13.
Physical Exam
Assessment of vital signs is a critical first step in differentiating between low risk, submassive, and massive PE categories. Specifically, hypotension and hemodynamic instability define massive PE. In general, vital signs may be abnormal, but cannot be relied upon as a sensitive screening test for ruling out the diagnosis of PE. Presenting symptoms can be mild and may be absent even in cases of large PE14. Normalization of an initially abnormal vital sign should not be used to forgo further evaluation for PE in symptomatic patients with risk factors for PE15. Common presenting signs of PE per the PIOPED II data include: tachypnea (54%), calf or thigh swelling, erythema, edema, tenderness, palpable cords (47%), tachycardia (24%), rales (18%), decreased breath sounds (17%), an accentuated pulmonic component of the second heart sound (15%), jugular venous distension (14%), and fever mimicking pneumonia (3%)14.
Laboratory Testing and EKG
EKG and laboratory evaluation help differentiate low risk and submassive PE, specifically in that submassive PE is defined as PE with evidence of right heart strain, albeit no hemodynamic instability. EKG findings significantly more frequent in PE patients with fatal outcomes include atrial arrhythmias, T wave inversions, complete right bundle branch block, peripheral low voltage, pseudoinfarction pattern (Q waves) in leads III and aVF, and ST segment changes (elevation or depression) over the left precordial leads16.
Troponin and BNP are often ordered in ED on the undifferentiated patient presenting with chest pain, shortness of breath, or in the hemodynamically unstable or patient in cardiac arrest. In the patient with PE, elevated troponin and/or BNP are associated with worse prognosis17,18.
Imaging Evaluation
Plain chest radiography, while not sensitive for the diagnosis of PE, can have several findings that can provide clues to the diagnosis. Cardiomegaly, unilateral pleural effusions, elevated hemidiaphragm, pulmonary artery enlargement, atelectasis, or wedge infarction (Hampton’s Hump) can be seen in PE.
Bedside limited echocardiography can be especially useful in the critically ill patient who is unable to go to CT due to hemodynamic instability or peri-arrest. Findings suggestive of a PE include RV/LV End-Diastolic Diameter >1 in apical 4 chamber view, paradoxical septal systolic motion, visualized thrombus, McConnell’s Sign (right ventricular hypokinesis with sparing of the apex) suggest PE19,20.
Traditionally the diagnostic gold standard for PE is pulmonary angiography. It is, however, invasive, expensive, and carries its own morbidity and mortality risk of up to 6% and 0.5%, respectively. The safety and efficacy of less invasive imaging modalities such as CT pulmonary angiography and ventilation/perfusion imaging has made the use of traditional angiography rare. It is now mostly reserved for cases in which catheter directed therapy is planned19.
CT pulmonary angiography (CTPA) has emerged as the diagnostic imaging modality of choice in patients who are stable enough to go to CT scan, have no allergy to iodinated contrast, and have renal function that permits the administration of IV contrast. The sensitivity of CTPA is thought to be 84-94%, and its specificity is up to 99%. The patient must be able to lie still and flat for the scan, as poor image quality significantly reduces the detection rate of PE19.
Ventilation/perfusion (V/Q) imaging is suitable for those patients with allergy to iodinated contrast material who cannot undergo CTPA. Most of the studies regarding its use have been done on non-critically ill patients. The ventilation portion of the exam is difficult to perform in mechanically ventilated patients. When the study conditions are ideal, its accuracy approaches that of CTPA; however, the ease and availability of CTPA has made V/Q imaging a secondary modality19.
Treatment – Who Needs Systemic Thrombolysis?
The mainstay of treatment for pulmonary embolism is anticoagulation. FDA approved anticoagulants for PE include unfractionated heparin (UFH), low molecular weight heparin (LMWH), Coumadin (warfarin), fondaparinux, bivalirudin, argatroban, and the novel oral anticoagulants (NOACs) rivaroxaban, dabigatran, apixaban, and edoxaban. Traditionally, either UFH or LMWH were used as a bridge until a therapeutic INR target of 2-3 could be reached with oral administration of Coumadin. Fondaparinux, argatroban, and bivalirudin are alternatives for patients with an allergy to UFH/LMWH, or those with a documented history of heparin induced thrombocytopenia. Increasingly, the NOACs are being used as primary therapy, likely because of their ease of use, predictability, and lack of need for intensive laboratory monitoring as compared with Coumadin21.
Massive PE
Evidence to support systemic thrombolysis in massive PE is found in multiple studies. A 2004 meta-analysis of 748 patients by Wan et al, evaluated systemic thrombolytics with anticoagulation vs placebo and anticoagulation. This study demonstrated a reduction in death or recurrent PE (9.4% vs.19.0%; NNT=10) in patients with major (hemodynamically unstable) pulmonary embolisms. Of note the thrombolytic group had a 10% absolute increase in major bleeding (NNH=10)22. The PEAPETT Trial from 2016 evaluated patients with PEA and cardiac arrest secondary to confirmed PE. 50mg of tPA IV push over one minute was administered to all patients. 22/23 patients attained ROSC, and 20/23 were still alive at a 2 year follow up. There was no reported major or minor bleeding complications20,23. Evidence based consensus guidelines from the European Society of Cardiology, the American College of Chest Physicians, and the American Heart Association recommend advanced antithrombotic therapies for patients with massive PE3,24,25. Systemic fibrinolysis has been shown to rapidly reduce thrombus burden, right ventricular dysfunction, and pulmonary vascular resistance. As a result, pulmonary capillary blood flow improves along with gas exchange26. Taken together, these benefits may provide rapid clinical improvement and in some cases prevent hemodynamic collapse21. However, true patient benefit is more controversial, and thrombolysis comes at the risk of increased bleeding.
Submassive PE
It is less clear which patients with submassive PE may derive benefit from systemic thrombolytics. The majority of investigation that has been done has considered submassive PE to be a single entity, whereas in reality this group may be more heterogeneous with some patients potentially benefitting from thrombolytics and others where the risks outweigh the benefits. Most studies are mixed and show some benefit to pulmonary perfusion and recurrence of venous thromboembolism, however most have failed to demonstrate a mortality benefit4. Thrombolytic doses and specific types also differ.
The Pulmonary Embolism Thrombolysis Trial (PEITHO) was a randomized double-blind design evaluating thrombolytics and heparin vs heparin alone in PE patients with normal systolic blood pressure, but with elevated troponin and right ventricular dilation. It demonstrated a 56% lower likelihood of death or hemodynamic decompensation in the thrombolytic/heparin group compared to the heparin only group (NNT 30)27. Chaterjee et al’s 2014 meta-analysis of 8 studies encompassing 1775 patients with either submassive or intermediate risk PE demonstrated an all-cause mortality decrease of 1.39% vs 2.92% with thrombolytics (NNT=65)28. It should be noted that both studies above also found that the benefits were offset by an elevated risk of major bleeding and hemorrhagic stroke. The thrombolytic group in the PEITHO had major bleeding in 11.5% vs. 2.4% (NNH=20) and ICH of 2.4% vs. 0.2% (NNH=46). The meta-analysis found the risk of major bleeding and hemorrhagic stroke to be 9% and 2% respectively27,28. Other analyses such as the International Cooperative PE Registry have found rates as high as 21% for major bleeding and 3% for fatal intracranial hemorrhage4. A randomized controlled trial of normotensive patients with submassive PE and evidence of right ventricular dysfunction demonstrated benefit from systemic thrombolytics on a combined endpoint of mortality and clinical features, such as requirement for escalation of therapy (intubation, vasopressor need, embolectomy, cardiopulmonary arrest), however there was no mortality benefit at 30 days29.
Perhaps adding to the confusion, in 2017 PEITHO conducted a long-term follow up of their original 2014 study on submassive PE patients. Long-term (median 37.8 months) survival was assessed in 353 of 359 (98.3%) patients in the thrombolysis arm and in 343 of 350 (98.0%) in the placebo arm. Overall mortality rates were 20.3% and 18.0%, respectively (p = 0.43). There was also no statistically significant difference in markers of morbidity (residual dyspnea, functional limitations, and persistent RV dysfunction)30.
Additionally, the consensus guidelines do not give uniform recommendations in cases of submassive PE. The American College of Chest Physicians recommends against systemic thrombolysis in submassive PE. The American College of Emergency Physicians finds insufficient evidence to recommend for or against the practice31. The American Heart Association and the European Society of Cardiology recommend it in selected patients. According to the American Heart Association selected patients include those who demonstrate clinical evidence of adverse prognosis (new hemodynamic instability, worsening respiratory insufficiency, severe RV dysfunction, or major myocardial necrosis) and low risk of bleeding complications (Class IIb; Level of Evidence C)3. The European Society of Cardiology is less specific recommending that thrombolytic use in submassive PE is not routine, but may be considered in select patients after thoroughly considering the bleeding risks31.
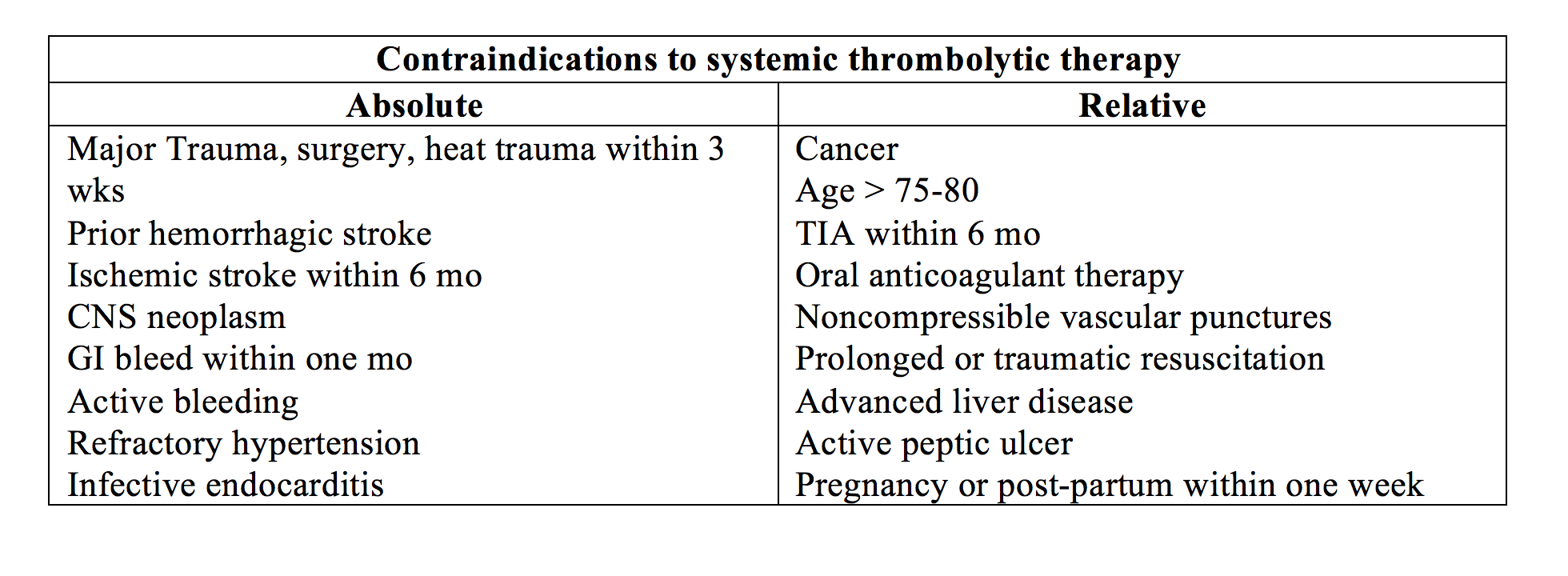
Carefully selected patients with submassive PE, including those with evidence of right heart dysfunction including RV dilation on echocardiography or CT, or those with elevated troponin I indicating right ventricular myonecrosis, may benefit from systemic thrombolytics in terms of speed to resolution, prevention of recurrent PE, and chronic thromboembolic pulmonary hypertension. The contraindications to systemic thrombolytics used as criteria in most studies are similar to those used in in ischemic stroke, and generally deal with risk of major or potentially fatal bleeding. For the emergency physician, it is clear that patients with massive PE without contraindications should be treated with systemic thrombolytics. Patients with submassive PE are by-definition hemodynamically stable and therefore more time can be taken for a discussion of risks and benefits with the patient, family, and admitting physicians to determine a best course of action. Risk of hemorrhage also requires consideration, as older patients demonstrate greater risk.
In addition to full dose thrombolysis, it is note-worthy that half-dose thrombolysis has been proposed as a strategy to provide benefit to PE and reduce bleeding complications. Trials studying half-dose thrombolysis in PE compared to standard anticoagulation found a reduction in surrogate outcomes including chronic pulmonary hypertension and clot burden on V/Q scan with lower rates of bleeding complications (especially in pts <65 yrs of age), however no mortality benefit31,32. Trials directly comparing half-dose to full-dose thrombolysis found a tendency toward lower bleeding complications in the half-dose strategy and no difference in mortality outcomes between the two treatment arms. A meta-analysis of trials comparing full-dose, half-dose, and standard anticoagulation found similar treatment efficacy of a half-dose strategy with lower rates of significant bleeding compared to full-dose33.
A full discussion of catheter directed therapies and surgical embolectomy is beyond the scope of this review, however they deserve brief mention. Catheter directed therapies may be utilized for those patients with contraindications to systemic thrombolytics, or those in whom systemic thrombolytics have failed. Catheter directed therapies can employ a combination of both mechanical clot disruption and evacuation and local thrombolytic delivery to avoid systemic effects. Surgical embolectomy, while traditionally employed as a last resort in peri-arrest patients, has become safer since the 1990’s, and is utilized more frequently in a broader range of patients. It can be considered in patients with contraindications to systemic thrombolytics or those in whom thrombolytics have failed34.
On a final note over the last several years numerous hospitals have developed Pulmonary Embolism Advanced Care Teams (PEAC) in order to more effectively treat hemodynamically unstable patients with confirmed PE. One of the first of these teams was started in 2013 at New York-Presbyterian/ Weill Cornell Medical Center. The team is comprised of a pulmonary/critical care physician, a cardiologist, an interventional radiologist, and a cardiothoracic surgeon. Their mission is to use a multi-disciplinary team approach to quickly identify patients who require treatment escalation, determine which thrombo-reductive strategy is most appropriate, and implement that strategy35.
Based on the available evidence the clinical bottom can be summarized as follows:
- Full-dose thrombolytics are effective and recommended in the treatment of massive PE, but carry a higher rate of serious and sometimes fatal bleeding complications, including intracranial hemorrhage.
- Full-dose thrombolytics may be considered in selected patients with submassive PE after a careful consideration and discussion of risks and benefits with the patient, family, and ICU consultant.
- Half-dose thrombolytics carries lower rates of serious bleeding complications and similar efficacy in surrogate outcomes to full-dose thrombolytics, however mortality data is limited.
- Consideration of the clinical status of the patient plays a significant role in determining the need for thrombolytics.
- Catheter directed treatment tends to be more expensive, is associated with longer ICU stays, and does not have as robust of evidence in support of its use, but may be an option for patients > 65 years of age and those in whom systemic thrombolytics would not be recommended.
- Surgical embolectomy remains an option in massive PE when less invasive strategies are contraindicated or ineffective.
Case Resolution
Your patient from the opening scenario remains hemodynamically stable throughout her stay in the ED. After the diagnosis is confirmed you begin anticoagulation with heparin and consult the intensivist for admission. After discussing risks and benefits with the patient and intensivist you elect to treat with anticoagulation alone for her submassive PE. The patient is admitted and has an uncomplicated hospital course beginning outpatient anticoagulation, and is discharged after several days.
Key Pearls
- Role of ED physician is first and foremost identification of PE and maintenance of a high index of suspicion as the diagnosis can be easily missed.
- Secondly, the ED physician is tasked with resuscitation and stabilization with particular attention paid to establishing the hemodynamic stability of the patient and categorizing them as low risk, submassive, and massive PE.
- Anticoagulation should be initiated as long as there are no contraindications once the diagnosis is strongly suspected, particularly with unfractionated heparin for patients in the submassive and massive PE category.
- For patients with massive PE which is defined as PE with hemodynamic instability, thrombolytics should be initiated given there are no contraindications.
- For patients with submassive PE, which by definition is hemodynamically stable, and evidence of right ventricular dysfunction, shared decision making should occur between the ED physician, patient, family, and admitting physicians regarding the risks and benefits of initiating systemic thrombolytics.
- For patients with massive PE and contraindications to systemic thrombolysis, catheter directed therapies or surgical embolectomy can be considered.
References/Further Reading
- Wood KE. Major Pulmonary Embolism. Crit Care Clin 2011; 27: 885-906.
- Fedullo P, Tapson V. Clinical practice. The evaluation of suspected pulmonary embolism. N Engl J Med. 2003;349(13):1247-1256.
- Jaff MR, McMurtry MS, Archer SL, et al; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788–1830.
- Goldhaber S, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353(9162): 1386-1389.
- Kreit J. The impact of right ventricular dysfunction on the prognosis and therapy of normotensive patients with pulmonary embolism. Chest. 2004;125(4):1539-1545.
- Stapczynski, J. S., & Tintinalli, J. E. (2011). Tintinalli’s emergency medicine: A comprehensive study guide(7th ed.). New York, N.Y.: McGraw-Hill Education LLC. pg. 431-440.
- Courtney DM, Kline JA, Kabrhel C et al.: Clinical features from the history and physical examination that predict the presence or absence of pulmonary embolism in symptomatic emergency department patients: results of a prospective, multicenter study. Ann Emerg Med 55: 305, 2010.
- PIOPED Investigators. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA 1990; 263:2753.
- Castelli R, Tarsia P, Tantardini C, et al. Syncope in patients with pulmonary embolism: comparison between patients with syncope as the presenting symptom of pulmonary embolism and patients with pulmonary embolism without syncope. Vasc Med 2003; 8:257.
- Well PS, et al. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001 Jul 17; 135(2): 98-107.
- Wolf SJ et al. Prospective validation of Wells Criteria in the evaluation of patients with suspected pulmonary embolism. Ann Emerg Med. 2004 Nov; 44(5): 503-10.
- Line JA, et al. Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. J Thromb Haemost 2004; 2: 1247-55.
- Kline JA, et al. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. J Thromb Haemost 2008; 6: 772-80.
- Stein PD, Beemath A, Matta F, et al. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am J Med 2007; 120:871.
- Kline JA, Corredor DM, Hogg MM, Hernandez J, Jones AE: Normalization of vital signs does not reduce the probability of acute pulmonary embolism in symptomatic emergency department patients. Acad Emerg Med 19: 11, 2012.
- Geibel A, Zehender M, Kasper W, et al. Prognostic value of the ECG on admission in patients with acute major pulmonary embolism. Eur Respir J 2005; 25:843.
- Becattini C et al. Prognostic Value of Troponins in Acute Pulmonary Embolism: A Meta-Analysis. Circulation 2007.
- Sanchez O et al. Prognostic Value of Right Ventricular Dysfunction in Patients with Hemodynamically Stable Pulmonary Embolism: A systematic Review. Eur Heart J 2008.
- Kline JA, et al. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. J Thromb Haemost 2008; 6: 772-80.
- Rezaie, Salim. The critical pulmonary embolism patient. Nov 11, 2016. http://rebelem.com/the-critical-pulmonary-embolism-patient/
- Rishi K et al. Treatment options in massive and submassive pulmonary embolism. Cardiology in Review 2016; 24: 19-25.
- Wan S et al. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation 2004; 110: 744-9.
- Sharifi M et al. Pulseless Electrical Activity in Pulmonary Embolism Treated with Thrombolysis (from the “PEAPETT” study). American Journal of Emergency Medicine 2016; 34: 1963 – 1967.
- Konstantinides SV. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35:3145–3146.
- Kearon C, Akl EA, Comerota AJ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S–e494S.
- Piazza G. Submassive pulmonary embolism. JAMA. 2013;309:171–180.
- Meyer G, Vicaut E, Danays T, et al; PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370:1402–1411.
- Chatterjee S, Chakraborty A, Weinberg I, et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014;311:2414–2421.
- Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002; 347(15):1143-1150.
- Konstantinides SV, Vicaut E, Danays T, et al. Impact of thrombolytic therapy on the long-term outcome of intermediate-risk pulmonary embolism. J Am Coll Cardiol 2017;69 1536-1544.
- Rezaie, Salim. Treatment of submassive pulmonary embolism: full dose, half dose, or no dose? Nov 3, 2016. http://rebelem.com/treatment-of-submassive-pe-full-dose-half-dose-or-no-dose/
- Sharifi M et al. Moderate Pulmonary Embolism Treated with Thrombolysis (from the “MOPETT” Trial). Am J Cardiol 2013; 111(2): 273 – 7.
- Zhang Z et al. Lower Dosage of Recombinant Tissue-Type Plasminogen Activator (rt-PA) in the Treatment of Acute Pulmonary Embolism: A Systematic Review and Meta-Analysis. Thrombosis Research 2014; 133(3): 357 – 63.
- Marshall, PS et al. Diagnosis and management of Life-Threatening Pulmonary Embolism. Journal of Intensive Care Medicine. 2011 26(5) 275-94.
- Sista AK, Friedman OA, Horowitz JM, Salemi A. Building a pulmonary embolism lysis practice: our strategy for assembling a team of specialists to provide efficient and effective acute PE care. Endovascular Today [Cover Story]. July 2013.








1 thought on “Pulmonary embolus in the ED – Which patients require systemic thrombolytics?”
Pingback: emDOCs.net – Emergency Medicine EducationTricuspid Annular Plane Systolic Excursion (TAPSE) for Risk Stratifying Patients with Pulmonary Embolism - emDOCs.net - Emergency Medicine Education