Authors: Aaron Lacy, MD (@AaronLacyMD, EM Resident Physician, Vanderbilt University Medical Center) and Clifford L. Freeman, MD (EM Attending Physician, Vanderbilt University Medical Center) // Reviewed by: Alexander Y. Sheng, MD, MHPE (@TheShenger); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case:
A 42-year-old male with a history of hypertension presents to your emergency department after a high-speed motor vehicle collision. EMS reports significant damage to the vehicle requiring extrication. Initial vitals include T 36.4°C, HR 112, BP 98/54, RR 22, SpO2 99% on room air. He is awake with repetitive questioning and is complaining of pain in his back and left hip. Primary survey is notable for an intact airway, bilateral breath sounds, weak radial pulse, and no obvious long bone deformities. A chest x-ray is unremarkable, and pelvis x-ray shows a left pubic ramus fracture. An E-FAST examination is negative. Your consultant resources include a general surgeon who is on-call, but not in-house.
Questions:
Where is the likely location of this patient’s bleeding? What advanced imaging can and should be obtained? What is your threshold to involve your on-call general surgeon, versus transfer to a comprehensive trauma center?
Background:
Abdominal-pelvic trauma remains the leading cause of morbidity and mortality in both children and adults aged 15-44 in the western world.1-3 Hemorrhagic shock must be assumed in patients presenting with hemodynamic instability after trauma until proven otherwise. A focused and expeditious workup must take place to identify the source of hemorrhage to provide definitive management.
Anatomic Locations of Potential Exsanguination
Thoracic Cavity
Abdominal Cavity – Peritoneal or retroperitoneal
Pelvic Cavity
Thighs
Scene (external exsanguination from laceration/injury)
In general, physical examination and abdominal laboratory testing are unreliable in detecting abdominal injuries, particularly in the retroperitoneum, as most bedside testing is directed at assessing the peritoneal space.1, 4 Classic physical examination signs of retroperitoneal bleeding, including Cullen’s, Turner’s,5 and Bryant’s sign,6, 7 are unlikely to be present in the acute setting. ATLS protocols allow for rapid identification of most areas of potential hemorrhage with chest and pelvic radiography in combination with E-FAST. Unfortunately, this approach is not designed to accurately assess for retroperitoneal bleeding. Retroperitoneal bleeding is important to identify even in patients without hemodynamic instability, as the retroperitoneum can be a source of clinically significant occult blood loss in the trauma patient, and delay in diagnosis is associated with higher morbidity and mortality.4, 8
Post-traumatic hemodynamic instability with no other signs of bleeding should be assumed secondary to retroperitoneal hemorrhage until proven otherwise.9
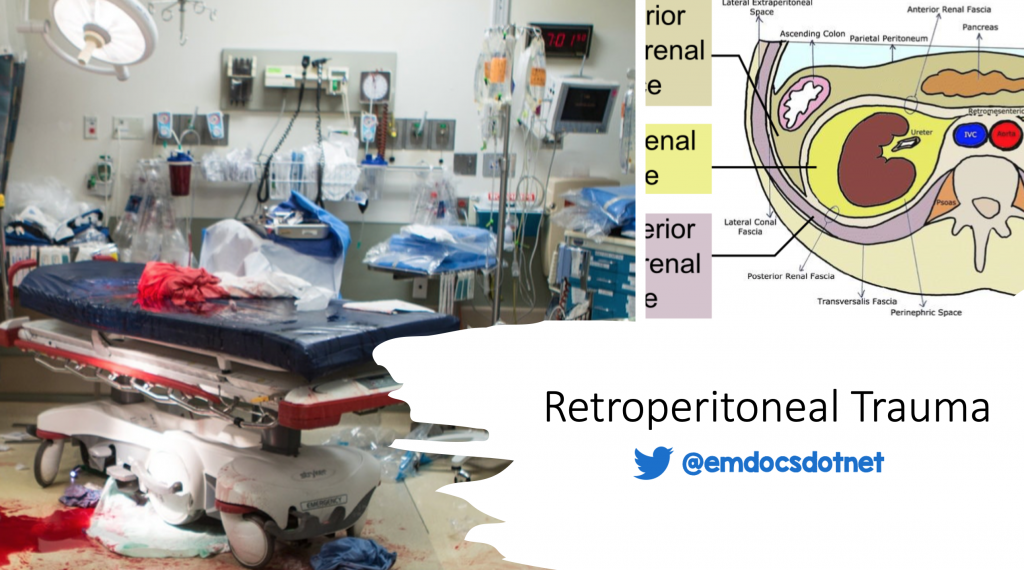
The retroperitoneum is a wide space lying posterior to the peritoneal cavity bounded posteriorly by the transversalis fascia and extends from the diaphragm to the pelvic inlet.4, 10 It contains a number of clinically significant visceral and vascular structures in the gastrointestinal, genitourinary, vascular, musculoskeletal, and nervous systems.10 Retroperitoneal hemorrhage is most often caused by blunt trauma,1-3, 9, 11 but in both blunt and penetrating trauma there is a high incidence of polytrauma.4, 10, 12-14 Reported rates of retroperitoneal hematoma after abdominal-pelvic trauma range from 12-30%,4, 10 with a wide reported range or mortality rates, 4-60%.14, 15 The most commonly injured solid organ injury is renal injury in both abdominal and penetrating injury.4 If retroperitoneal trauma is associated with hollow viscous injury the prognosis is grim.4, 16
Retroperitoneal bleeding can be divided into three anatomical zones.4, 10
Zone 1: midline between aortic hiatus and sacral promontory
- Highest risk for vascular injury10, 17
Zone 2: Flank or lateral retroperitoneum
- Second most common area of bleeding, most likely from a renal source1, 2, 4
Zone 3: Pelvic retroperitoneum
- Most common location of hemorrhage4, 15
- Frequently associated with pelvic fractures2, 9

Treatment selection is heavily dependent on the zone involved. Zone 1 injuries almost always require surgical intervention, while zone 2 and 3 injuries can be managed differently based on anatomical structures involved and the patients hemodynamic status. Pelvic ring fractures, which cause hemorrhage in zone 3, are of particular concern given their high associated mortality rate.14, 18, 19 The pelvis is highly vascularized and venous injury (90%) is much more common over arterial injury (10%).9, 10, 14 Given that pelvic injuries are the most common cause of retroperitoneal hemorrhage and carry a high rate of shock and mortality,2, 14 suspicion for retroperitoneal hemorrhage should be high when signs of pelvic trauma are present. Mortality rate is high in those who suffer penetrating injuries,12 in particular those in zone 1, which puts the great vessels at risk.13, 17, 20
Evaluation and Management of Retroperitoneal Trauma
Evaluation of the trauma patient begins with standard practice following ATLS guidelines; with rapid assessment of airway, breathing, circulation, and disability.21 In patients who are hemodynamically unstable the transition towards resuscitation with blood products should be made quickly, as hemorrhagic shock is the most likely source.
The suspicion for retroperitoneal bleeding should be high in both trauma patients without signs of other obvious source of trauma, as well as in those with other sources of trauma, as retroperitoneal hemorrhage is present in up to a 1/3 of all polytrauma.10
Evaluation for signs of hemorrhage in the thoracic and peritoneal cavities can be done with both chest radiography and E-FAST performed by a trained provider.21 Given that zone 3 is the most common location of retroperitoneal trauma, and is frequently associated with pelvic ring fractures, pelvic radiography is an important step in the evaluation of the hemodynamically unstable trauma patient.8
In patients with presumed retroperitoneal trauma there are several options that can occur in the resuscitation bay by emergency physicians to facilitate patient resuscitation.
Pelvic binding – Good evidence
- In patients with visualized pelvic ring fracture or concerns for unstable pelvis on physical examination, the pelvis should be wrapped to help with hemorrhage control9
- When applied correctly, there has been no pelvic binding method found to be superior to one another22, 23
External Pelvic packing – Good evidence
- 10th edition ATLS guidelines suggest pre-peritoneal packing as a method for controlling pelvic hemorrhage19, 21
- This most often occurs in the operating room, but can be done at the bedside
REBOA – Unclear if useful
- REBOA can be considered in retroperitoneal hemorrhagic shock
- Evidence is lacking for improved morbidity and mortality,8, 14, 24 and the timing of its placement has still not been clarified2
ED left sided thoracotomy – Mixed evidence
- Must be ideal circumstance
- ED thoracotomy may bide time while getting patient to the operating room8
- In penetrating hemorrhagic trauma patients there is no improved survival in patients who undergo left sided thoracotomy20
Ultimately, all of these methods only provide a temporary solution. Patients with hemorrhagic shock from retroperitoneal bleeding require definitive management by interventional radiology or surgery.9
A management crossroads for patients with retroperitoneal hemorrhage is their hemodynamic stability. In trauma patients with concern for retroperitoneal hemorrhage and who are hemodynamically stable, the imaging and evaluation tool of choice is CT imaging.4, 9, 11, 14, 15, 17 Retroperitoneal hemorrhage is difficult to diagnose1, and clinically significant.4Maintaining a low threshold for CT imaging is essential to making the diagnosis. CT with IV contrast can most effectively evaluate the retroperitoneal organs and vasculature, and in hemodynamically stable patients will determine the route for definitive therapeutic management.17 Of course, CT scan should NOT delay or take the place of other resuscitative measures, including exploratory laparotomy.
In patients whose hemodynamics allow, CT imaging is critically important in the workup of retroperitoneal hemorrhage, both for diagnostic and therapeutic planning purposes.4, 9, 11, 14, 15, 17 However, it should not delay resuscitative measures, transfer, or operative management in those who are hemodynamically unstable.
Retroperitoneal bleeding ultimately requires definitive management via angioembolization (interventional radiology) or surgical repair. Interventional radiology was first used for management of retroperitoneal hemorrhage in 1972,25 and has slowly gained more prominence in subsequent decades as an effective option for hemorrhage control.2, 4, 15, 18Nevertheless, 24/7 in-house presence for interventional radiology is not a requirement for level 1-trauma centers in the United States, and availability is not ubiquitous among medical institutions.18 The role of interventional radiology versus surgery for definitive management ultimately depends on the mechanism of injury, injury location, and presence of hemodynamic instability.
While algorithms have been proposed for management of retroperitoneal trauma, they are not unified across different specialties, societies, or groups. In most algorithms the management escalates as clinical status worsens, ranging from observation, to angioembolization, to surgical intervention.
Despite the availability of interventional radiology versus specialized trauma surgical care to determine ultimate management, retroperitoneal injury in the trauma patient requires specialized, multidisciplinary care.4, 9, 11, 14, 19 These patients require a team-based approach including acute care physicians, nurses, clinical technicians, rehabilitation specialists and multiple types of interventionists or surgeons.
Retroperitoneal bleeding secondary to trauma requires a multidisciplinary team approach,4, 9, 11, 14, 19 and every effort should be made to facilitate transfer to a facility with the appropriate resources.9
In conclusion, the role of the ED provider in retroperitoneal trauma requires a high level of suspicion for retroperitoneal injury, appropriate resuscitation, and the recognition that a patient’s clinical status often determines the most appropriate workup and definitive care after initial stabilization.
Case Resolution
Our patient presented with borderline hypotension, tachycardia, and a GCS of 14. Given that he had a severe traumatic mechanism with decreased mentation concerning for end organ dysfunction the transition to blood product administration was expeditious. Since the workup thus far included a negative CXR, E-FAST, and a pelvic x-ray showing a pubic rami fracture, his hemorrhage was assumed to be coming from the retroperitoneal space.
The patient’s vital signs stabilized after administration of blood products. Consultation to the on-call surgeon was deferred to the decision to transfer the patient to a tertiary care trauma facility for definitive management. While ensuring that it would not delay transfer, a CT scan was obtained while awaiting a critical care transfer unit, showing renal lacerations and the known pubic rami fracture with a small amount of associated active extravasation in the pelvis. He underwent interventional radiology embolization at the tertiary care facility for hemorrhage control and continues to recover in their multidisciplinary trauma unit.
Pearls
- Trauma patients with hemodynamic changes with a negative chest x-ray, E-FAST, and pelvic x-ray should be presumed to have retroperitoneal trauma until proven otherwise.
- The most common cause of retroperitoneal trauma is secondary to zone 3 injuries in the pelvis. Use pelvic binders to stabilize pelvic ring fractures at the bedside, and rapid transition to extra-peritoneal packing to reduce further hemorrhage.
- Once the patient is stable enough for CT, obtaining CT with IV contrast is critical to diagnosing and evaluating the source of retroperitoneal hemorrhage.
- Patients with hemodynamic instability and retroperitoneal hemorrhage require either interventional radiology or surgical specialist intervention for definitive care.
- Any type of retroperitoneal hemorrhage requires multidisciplinary care, no matter the patient’s hemodynamic instability.
References:
- El-Menyar, A., Abdelrahman, H., Al-Thani, H., Zarour, A., Parchani, A., Peralta, R., and Latifi, R. Compartmental anatomical classification of traumatic abdominal injuries from the academic point of view and its potential clinical implication. Journal of Trauma Management and Outcomes. 2014. 8:14.
- Ptohis, N., Charalampopoulos, G., Alie, A., Avgerinos, E., Mousogianni, I., Filippiadis, D., Karydas, G., Gravanis, M., and Pagoni, S. Contemporary role of embolization of solid organ and pelvic injuries in polytrauma patients. Frontiers in Surgery. 2017. 4:43.
- Miele, V., Piccolo, C., Trinci, M., Galluzzo, M., Ianniello, S., and Brunese, L. Diagnostic imaging of blunt abdominal trauma in pediatric patients. 2016. Radiology Med. 121:409-430.
- Daly, K., Ho, C., Persson, D., and Gay, S. Traumatic retroperitoneal injuries: review of multidetector CT findings. RadioGraphics. 2008. 28:1571-1590.
- Mookadam, F. and Sikes, M. Cullen’s and Turner’s signs. New England Journal of Medicine. 2005. 353(13):1386.
- Ratzan, R., Donaldson, M., Foster, J., and Walzak, M. The blue scrotum sign of Bryant: a diagnostic clue to ruptured abdominal aortic aneurysm. Journal of Emergency Medicine. 1987;5(4):323-329.
- Campo, I., Valenitino, M., Sidhu, P., Meconi, L., Niewenhove, S., Cova, M., Derchi, L., and Bertolotto, M. Nonscrotal causes of acute scrotum. Journal of Ultrasound Medicine. 2020. 9999:1-9.
- Stahel, P., Burlew, C., and Moore, E. Current trends in the management of hemodynamically unstable pelvic ring injuries. Current Opinions in Critical Care. 2017. 23:511-519.
- Geeraerts, T., Chhor, V., Cheisson, G., Martin, L., Bessoud, B., Ozanne, A., and Duranteau, J. Clinical review: initial management of blunt pelvic trauma patients with haemodynamic instability. Critical Care. 2007. 11:204.
- Manzini, N., and Madiba, T. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury. 2014. 45:1378-1383.
- Feliciano, D. Management of traumatic retroperitoneal hematoma. Annals of Surgery. 1990. 211(2):109-123.
- Voelzke, B., and McAninch, J. Renal Gunshot Wounds: Clinical Management and Outcome. Journal of Trauma. 2009. 66:593-601.
- Bochicchio, G. Treatment of the bleeding in the urban battlefield. Surgery. 2007;142:S78-S83.
- Watkins, R., and Hsu, J. The road to survival for haemodynamically unstable patients with open book pelvic fractures. Frontiers in Surgery. 2020. 7:58.
- Wang, F., and Wang, F. The diagnosis and treatment of traumatic retroperitoneal hematoma. Pak J Med Sci. 2013. 29(2):573-576.
- Lai, C., Huang, H., and Chen, R. Combined stomach and duodenal perforating injury following blunt abdominal trauma: a case report and literature review. BMC Surgery. 2020. 20:217.
- Chapellier, X., Sockeel, P., and Baranger, B. Management of penetrating abdominal vessel injuries. Journal of Visceral Surgery. 2010. 147:e1-e12.
- Papkostidis, C., Kanakaris, N., Dimitriou, R., and Gianoudis, P. The role of arterial embolization in controlling pelvic fracture haemorrhage: a systemic review of the literature. European Journal of Radiology. 2012. 81:897-904.
- Osborn, P., Smith, W., Moore, E., Cothren, C., Morgan, S., Williams, A., and Stahel, P. Direct retroperitoneal pelvic packing versus pelvic angiography: A comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury. 2009. 40:54-60.
- Smith, S. Traumatic retroperitoneal venous haemorrhage. British Journal of Surgery. 1988. 75:632-636.
- Galvagno, S., Nahmias, J., and Young D. Advanced trauma life support update 2019: Management and applications for adults and special populations. Anesthesiol Clin. 2019. 37(1): 13-32.
- Knops, S., Schep, N., Spoor, C., van Riel, M., Spanjersberg, W., Kleinrensink, G., van Lieshout, E., Patka, P., and Schipper, I. Comparison of three different pelvic circumferential compression devices: a biomechanical cadaver study. Journal of Bone Joint Surgery of America. 2011. 93(3):230-240.
- Knopws, S., Van Lieshout, E., Spanjersberg, W., Patka, P., and Schipper, I. Randomised clinical trial comparing pressure characteristics of pelvic circumferential compression devices in healthy volunteers. Injury. 2011. 42(10):1020-1026.
- Biffl, W., Fox, C., and Moore, E. The role of REBOA in the control of exsanguinating torso hemorrhage. Journal of Trauma and Acute Care Surgery. 2015. 78(5):1054-1058.
- Salcedo, E., Brown, I., Corwin, M., and Galante, J. Pelvic angioembolization in trauma – indications and outcomes. International Journal of Surgery. 2016. 33:231-236.




