Author: Courtney Cassella, MD (EM Resident Physician, Icahn School of Medicine at Mount Sinai)
Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
Definition: Transient loss of consciousness with spontaneous recovery
Clinical Scenario: A 67 year-old man with a past medical history of hypertension and diabetes presents to the emergency department with syncope. The patient was taking a walk with his wife when he passed out. He was unconscious for 1 minute with no rhythmic jerking, tongue biting, or loss of bladder function. Initial vital signs are T 98.6 P 49 BP 146/63 RR 16, O2 sat 98% on RA. Physical exam is within normal limits. ECG is sinus bradycardia with T-wave flattening in II, III, and AVF.
Classification and Clues in the History 1-5
A discussion on the latest clinical work-up and management of syncope would not be complete without a general overview of the etiologies of syncope. For in-depth reading of vascular syncope please see this prior emDocs post: http://www.emdocs.net/vascular-causes-of-syncope/.
- Reflex or Neurally Mediated
- Heterogeneous group consisting of various provoking stimuli leading to hypotension and vasodilation with relative bradycardia
- Differentiating Features
- Prodrome: warmth, diaphoresis, nausea, dyspnea, ringing in the ears, abdominal pain, fatigue
- Syncope at rest, after exercise
- Brief LOC (<5 min)
- Vasovagal – strong emotion or physical pain
- Pain, medical procedures, prolonged standing, hot or crowded situations, valsalva, strong emotion
- Situational – distension of hollow viscera (esophagus, rectum, bladder)
- Cough, micturition, defecation, swallowing, vomiting
- Carotid sinus – seen in the elderly; neck stretching or shaving
- Orthostatic Hypotension Mediated
- Orthostatic stress followed by insufficient peripheral vasoconstriction
- Classified by within 3 minutes of standing
- Decrease in Systolic blood pressure >20 mmHg
- Decrease in Diastolic blood pressure >10 mmHg
- Investigate
- Acute hemorrhage
- Gastrointestinal bleeding
- Menstrual bleeding/Ectopic pregnancy
- Abdominal Aortic Aneurysm with leak/rupture
- Septic Shock, Distributive Shock (such as anaphylaxis)
- Excessive diuresis, diarrhea, vomiting
- Addison’s disease
- Acute hemorrhage
- Aggravated by
- Medication use
- Advancing age
- Diabetes mellitus
- Primary autonomic dysfunction – Parkinson’s, Lewy body dementia
- Cardiovascular Mediated
- Differentiating Features
- Brief or absent prodrome
- May be preceded by palpitations
- Syncope at rest or with exertion
- Brief LOC (<5 min)
- Rapid recovery
- Dysrhythmia
- Long QT Syndrome
- Brugada Syndrome
- Pre-excitation (such as WPW)
- Ventricular tachycardia
- Torsades de pointes
- Supraventricular tachycardia
- Atrial fibrillation/flutter
- Second or Third degree AV block
- Sick sinus syndrome
- Structural
- Valvular heart disease – aortic, mitral, or tricuspid stenosis
- Hypertrophic cardiomyopathy
- Pulmonary embolism
- Pericardial tamponade
- Myocardial Infarction
- Aortic dissection
- Subclavian steal syndrome
- Severe congestive heart failure
- ACEP Level A rec: Use H&P to identify HF patients at risk6
- Congenital heart disease
- Myxoma
- Non-syncopal Transient Loss of Consciousness
- Seizures
- Posturing, head turning, tongue biting, rhythmic limb jerking, eye deviation
- Post-ictal confusion/state
- Vertebrobasilar TIA
- Subarachnoid hemorrhage
- Headache, altered mental status, focal neurologic deficits
- Subdural/epidural hemorrhage, traumatic brain injury
- Metabolic
- Most metabolic etiologies will have prolonged LOC or less likely to resolve without intervention
- Medication/drug overdose
- Hypoglycemia
- Hypoxia/hyperventilation
Additional History
- Activity, events surrounding syncope, prodrome, trauma with event
- Medications, exposures (CO poisoning), drugs of abuse
- Family history of syncope or untimely death
Physical Examination
- Vital signs for heart rate, blood pressure
- Orthostatics
- Head: Signs of head trauma
- Neck: Assess for c-spine tenderness secondary to trauma from syncope, jugular venous distension
- Cardiovascular: Assess for murmurs, signs of cyanosis
- Abdomen: Pulsating mass
- Digital rectal examination for bleeding
- Neurologic: Assess for focal deficits
All syncope work-ups and syncope clinical decision rules start with the same basic information, history, physical, and an ECG.
- ECG for all patients 6
- Evidence of ischemia/infarct
- HOCM
- Prolonged QT interval
- Brugada pattern
- Pre-excitation – delta wave, short PR
- Conduction disturbances – bundle branch/fascicular blocks, second or third degree AV block
- Serum/Urine pregnancy test for all women of child-bearing age
- Finger stick glucose
The decision to draw labs is dependent on patient risk factors and need for additional information. Per ACEP clinical policy, younger patients with non-exertional syncope and no history of cardiovascular disease, family history of sudden death, or comorbidities are low risk of adverse events.6 In this population, it may be possible to forgo additional blood testing.
- Consider
- CBC for hematocrit
- BMP for electrolytes
- Troponin
- BNP – Brain natriuretic peptide
- Stool fecal occult blood
- Clinical judgment and/or defer to inpatient evaluation
- Holter monitor / Stress test
- Aortic Ultrasound
- Echocardiography
- Computed Tomography of the head
- Electroencephalogram
Decision Rules
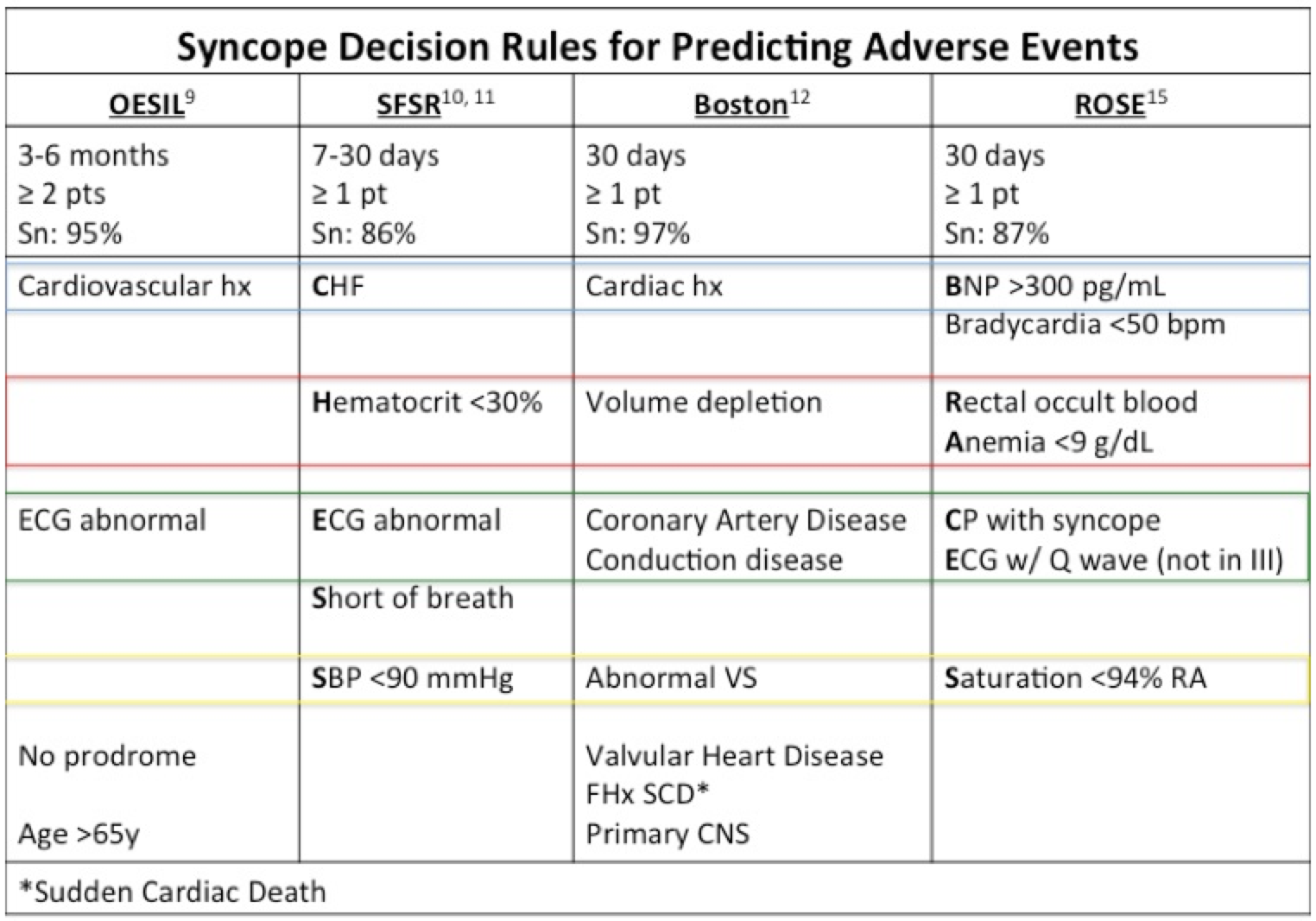
There has been a tremendous effort to derive and validate decision rules to identify patients at high risk for adverse outcomes and secondarily define those needing inpatient admission. According to two meta-analyses,7, 8 only the Osservatorio Epidemiologico sulla Sincope nel Lazio (OESIL) risk score9 and San Francisco Syncope Rule (SFSR)10, 11 have been externally studied. There are several additional rules including but not limited to the Boston Syncope Criteria,12, 13 Risk stratification of Syncope in the Emergency Department (ROSE),14, 15 and Evaluation of Guidelines in Syncope Study (EGSYS) score.16 Unfortunately, neither externally studied decision rule, OESIL or SFSR, has proven reliable for routine use in clinical practice. The limitations of both rules will be discussed below.
Osservatorio Epidemiologico sulla Sincope nel Lazio (OESIL) risk score7-9, 17, 18
There are two issues with using the OESIL for risk stratification by the emergency provider. First, the OESIL pooled data for “low risk” for adverse outcomes was inconsistent across studies ranging from 5-13% adverse events. These results could not be explained or adjusted for by differences in the studied outcome period. Furthermore, the OESIL aims to predict adverse outcomes in 3-6 months and was initially studied in adverse outcomes at 1 year. Although clinically significant for patients overall, for the emergency provider adverse outcomes at 3 months to 1 year only minimally aid in the decision between admission or close outpatient follow-up.
- ≥2 points: Pooled sensitivity was 95%7 and 78%8 in predicting adverse outcomes at 3-6 months and 10 days, respectively.
- Age >65
- History of cardiovascular disease
- Syncope without prodrome
- Abnormal ECG
San Francisco Syncope Rule (SFSR)7, 8, 10, 11, 17, 19, 20
The SFSR is ideal for emergency physician decision by studying adverse outcomes in 7 days. Despite early internal sensitivity of 98%,10 pooled sensitivity is a disappointing 86%. Some suspect the definition of ECG abnormality and varying patient populations leads to the variation in sensitivity.7, 21 The derivation rule defines abnormal ECG as any non-sinus rhythm or new changes in comparison to previous ECG. If there is no old ECG, then any rhythm that is not sinus is considered abnormal.
Perhaps the most useful application of the SFSR would be in patients with no evident cause of syncope after initial evaluation. A 2011 systematic review by Saccilotto et al found the probability of serious outcome with a negative CHESS score was reduced from 5% to lower than 2% if applied to patients without an evident cause of syncope.20
- Pooled sensitivity was 86%,7 primarily studied in predicting adverse outcomes at 7 days.
- CHESS – 1 point: high risk for serious outcome
- C – Congestive Heart Failure (history of)
- H – Hematocrit <30%
- E – ECG abnormal
- S – Shortness of breath
- S – Systolic BP at triage of <90 mmHg
Practice Guidelines
There are several agencies including ACEP, CCS, and ECS with published clinical policies or guidelines. As with clinical decision tools, the major high risk factors are similar.
ACEP Clinical Policy, 20096
- Level B: Consider younger patients with non-exertional syncope, without history of cardiovascular disease, family history of sudden death, or comorbidities low risk of adverse events.
- Level B: Admit with high risk factors for adverse outcome
- Older age and associated comorbidities
- Abnormal ECG – acute ischemia, dysrhythmias, significant conduction abnormalities
- Hematocrit <30%
- History or presence of heart failure, CAD, or structural disease
Canadian Cardiac Society Guidelines, 2011:22 High-risk features for adverse events
- Abnormal ECG: Any tachyarrhythmia, bradyarrhythmia, conduction disease, new ischemia or old infarct
- History of cardiac disease: ischemic, arrhythmic
- Hypotension: Systolic <90 mmHg
- Heart failure: Current or past
- Minor risk factors (urgent assessment):
- Age >60
- Dyspnea
- Anemia (Hematocrit <30%)
- Hypertension
- Cerebrovascular disease
- Family history of sudden cardiac death (<50y)
- Specific situation – syncope during exertion, while supine, or without prodrome
European Society of Cardiology Guidelines, 2009:4 High-risk criteria requiring prompt hospitalization or intensive evaluation
- Severe structural or coronary artery disease – heart failure, low LVEF, previous MI
- Clinical or ECG features suggesting arrhythmic syncope
- Syncope during exertion or supine, palpitations
- Family history of sudden cardiac death
- Arrhythmias
- Severe anemia
- Electrolyte disturbance
Emergency Department Disposition
In patient’s presenting with syncope, the most pertinent question in management is, does the patient need an inpatient admission or observation for additional investigation?
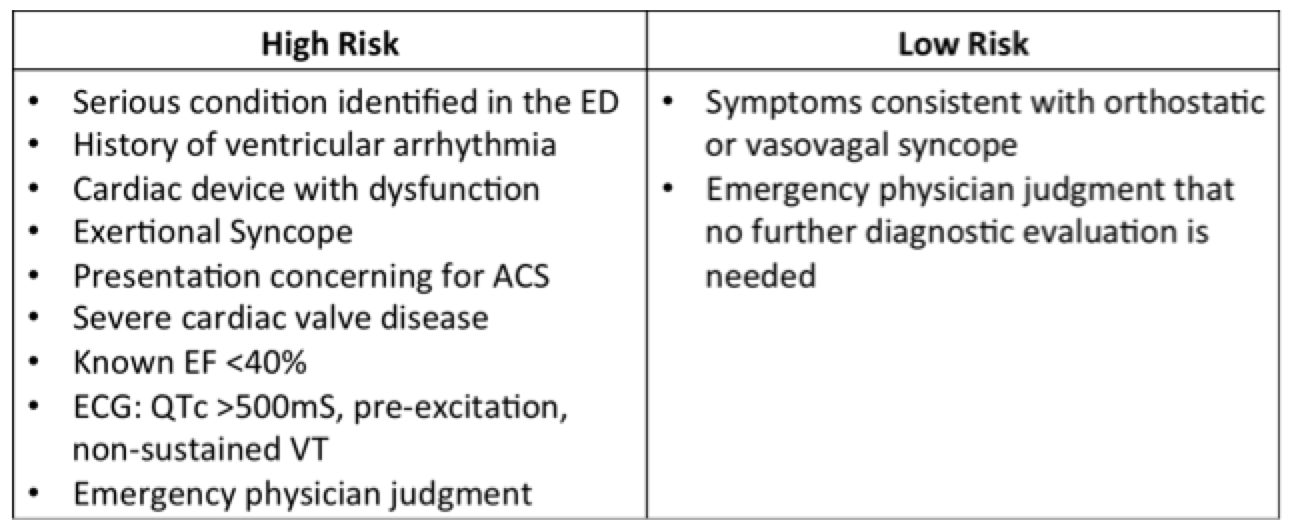
Low risk patients, as identified by ACEP Clinical policy,6 may be considered for discharge with prompt outpatient follow-up. In a RCT by Sun et al,23 intermediate risk patients were randomized to inpatient admission versus observation unit. Intermediate patients were those older than 50 years with no high or low risk features (see table below). The study found intermediate risk patients could undergo an observation period with similar serious outcomes to admission at 40 days. The observation period consisted of at least 12 hours of cardiac monitoring, 2 serial troponins, and an echocardiogram for those with a murmur or no echo within 6 months.
In determining high-risk patients, clinical decision rules alone are not reliable for clinical practice.7, 8 A 2014 meta-analysis by Costantino et al compared the OESIL, SFSR, and EGSYS prediction tools with clinical judgment. The paper found clinical judgment had a sensitivity of 95% versus clinical decision rules sensitivity of 63-78% in predicting serious outcomes at 10 days. This data does not support the use of only clinical judgment, but sheds light on the inconsistency of clinical decision rules. However, clinical decision rules, medical society guidelines, and clinical judgment can help direct the emergency physician to high-risk patients requiring admission. Common red flags include from CDR and the literature include:
- Abnormal ECG
- Abnormal vital signs
- Hypotension SBP <90 mmHg
- Bradycardia <50 bpm
- O2 saturation <94%
- History of cardiac disease
- CHF
- Structural
- Ischemia
- Arrhythmia
- Anemia
- Hematocrit <30% or Hemoglobin <9g/dL
- Older age >60 years
References / Further Reading
- Saklani P, Krahn A, Klein G. Syncope. Circulation. 2013;127(12):1330-1339.
- Peeters SY, Hoek AE, Mollink SM, Huff JS. Syncope: risk stratification and clinical decision making. Emergency medicine practice. 2014;16(4):1-22; quiz 22-23.
- Transient Loss of Consciousness (‘Blackouts’) Management in Adults and Young People. London2010.
- Task Force for the D, Management of S, European Society of C, European Heart Rhythm A, Heart Failure A, Heart Rhythm S, et al. Guidelines for the diagnosis and management of syncope (version 2009). European heart journal. 2009;30(21):2631-2671.
- Long B. Vascular Causes of Syncope. Practice Updates. http://www.emdocs.net/vascular-causes-of-syncope/. Published 2015. Accessed August, 1, 2015.
- Huff JS, Decker WW, Quinn JV, Perron AD, Napoli AM, Peeters S, et al. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Annals of emergency medicine. 2007;49(4):431-444.
- Serrano LA, Hess EP, Bellolio MF, Murad MH, Montori VM, Erwin PJ, et al. Accuracy and quality of clinical decision rules for syncope in the emergency department: a systematic review and meta-analysis. Annals of emergency medicine. 2010;56(4):362-373 e361.
- Costantino G, Casazza G, Reed M, Bossi I, Sun B, Del Rosso A, et al. Syncope risk stratification tools vs clinical judgment: an individual patient data meta-analysis. The American journal of medicine. 2014;127(11):1126 e1113-1125.
- Colivicchi F, Ammirati F, Melina D, Guido V, Imperoli G, Santini M, et al. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: the OESIL risk score. European heart journal. 2003;24(9):811-819.
- Quinn J, McDermott D, Stiell I, Kohn M, Wells G. Prospective validation of the San Francisco Syncope Rule to predict patients with serious outcomes. Annals of emergency medicine. 2006;47(5):448-454.
- Quinn JV, Stiell IG, McDermott DA, Sellers KL, Kohn MA, Wells GA. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Annals of emergency medicine. 2004;43(2):224-232.
- Grossman SA, Bar J, Fischer C, Lipsitz LA, Mottley L, Sands K, et al. Reducing admissions utilizing the Boston Syncope Criteria. The Journal of emergency medicine. 2012;42(3):345-352.
- Grossman SA, Fischer C, Lipsitz LA, Mottley L, Sands K, Thompson S, et al. Predicting adverse outcomes in syncope. The Journal of emergency medicine. 2007;33(3):233-239.
- Reed MJ, Newby DE, Coull AJ, Prescott RJ, Jacques KG, Gray AJ. The ROSE (risk stratification of syncope in the emergency department) study. Journal of the American College of Cardiology. 2010;55(8):713-721.
- Reed MJ, Newby DE, Coull AJ, Jacques KG, Prescott RJ, Gray AJ. The Risk stratification Of Syncope in the Emergency department (ROSE) pilot study: a comparison of existing syncope guidelines. Emergency medicine journal : EMJ. 2007;24(4):270-275.
- Del Rosso A, Ungar A, Maggi R, Giada F, Petix NR, De Santo T, et al. Clinical predictors of cardiac syncope at initial evaluation in patients referred urgently to a general hospital: the EGSYS score. Heart. 2008;94(12):1620-1626.
- Dipaola F, Costantino G, Perego F, Borella M, Galli A, Cantoni G, et al. San Francisco Syncope Rule, Osservatorio Epidemiologico sulla Sincope nel Lazio risk score, and clinical judgment in the assessment of short-term outcome of syncope. The American journal of emergency medicine. 2010;28(4):432-439.
- Hing R, Harris R. Relative utility of serum troponin and the OESIL score in syncope. Emergency medicine Australasia : EMA. 2005;17(1):31-38.
- Thiruganasambandamoorthy V, Hess EP, Alreesi A, Perry JJ, Wells GA, Stiell IG. External validation of the San Francisco Syncope Rule in the Canadian setting. Annals of emergency medicine. 2010;55(5):464-472.
- Saccilotto RT, Nickel CH, Bucher HC, Steyerberg EW, Bingisser R, Koller MT. San Francisco Syncope Rule to predict short-term serious outcomes: a systematic review. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2011;183(15):E1116-1126.
- Thiruganasambandamoorthy V, Stiell IG, Sivilotti ML, Murray H, Rowe BH, Lang E, et al. Risk stratification of adult emergency department syncope patients to predict short-term serious outcomes after discharge (RiSEDS) study. BMC emergency medicine. 2014;14:8.
- Sheldon RS, Morillo CA, Krahn AD, O’Neill B, Thiruganasambandamoorthy V, Parkash R, et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. The Canadian journal of cardiology. 2011;27(2):246-253.
- Sun BC, McCreath H, Liang LJ, Bohan S, Baugh C, Ragsdale L, et al. Randomized clinical trial of an emergency department observation syncope protocol versus routine inpatient admission. Annals of emergency medicine. 2014;64(2):167-175.
- http://www.ncbi.nlm.nih.gov/pubmed/25943042
- http://www.ncbi.nlm.nih.gov/pubmed/26204970





2 thoughts on “Syncope: The Latest on Clinical Work-up and Management”
Pingback: Syncope: The Latest on Clinical Work-up and Management – emdocs – Skinny white coat
Pingback: emDOCs.net – Emergency Medicine EducationElemental EM: Eating Disorders - emDOCs.net - Emergency Medicine Education