
Author: Michael J. Yoo, MD (Assistant Professor/Core Faculty, San Antonio, TX) // Reviewed by Brit Long, MD (@long_brit)
Case
An 18-year-old man with a history of asthma and medication noncompliance presents to the emergency department (ED) with acute onset shortness of breath. He states that he recently moved to Texas from Colorado. His initial vital signs are 126/83 mmHg, heart rate of 104 beats per minute, respiratory rate of 32 breaths per minute, and saturation of 92% on room air. He is afebrile. The physical exam is notable for diffuse inspiratory and expiratory wheezing, consistent with acute asthma exacerbation. You treat him with nebulized therapies and decide to initiate systemic steroids. Your asthma order set has several options: dexamethasone, prednisone, prednisolone, and methylprednisolone. Which one do you select?
Background
Systemic steroids are commonly used and prescribed from the emergency department (ED). While their efficacy may be controversial in certain conditions, systemic steroids are used in nearly every organ system. In the ED, we are primarily interested in their effects on inflammation and sodium and fluid retention, though systemic steroids are also commonly used for their immunosuppressive and anti-proliferative properties.1 When discussing the anti-inflammatory and sodium retention characteristics of steroids, we are specifically referring to their glucocorticoid and mineralocorticoid potency, respectively. Activation of the glucocorticoid receptor has an inhibitory effect on the enzyme phospholipase A2, with subsequent decreases in pro-inflammatory cytokines, prostaglandins, and at higher doses, B-cell and T-cell production.2-3 Furthermore, mineralocorticoid receptors play a direct role in increasing the sodium-potassium exchange activity and water retention in the kidneys.2-3 The presence of mineralocorticoid receptors on endothelial and vascular smooth muscle cells also allows for vasoconstriction when they are activated.5
ED physicians often reach for dexamethasone or prednisone, but what are their properties? Are they primarily glucocorticoids, mineralocorticoids, or both? What is the duration of action of these steroids? We discuss the differences between systemic steroids below (Table 1). For the scope of this article, we will limit our discussion to systemic steroids and not include inhaled, topical, or intranasal steroids.
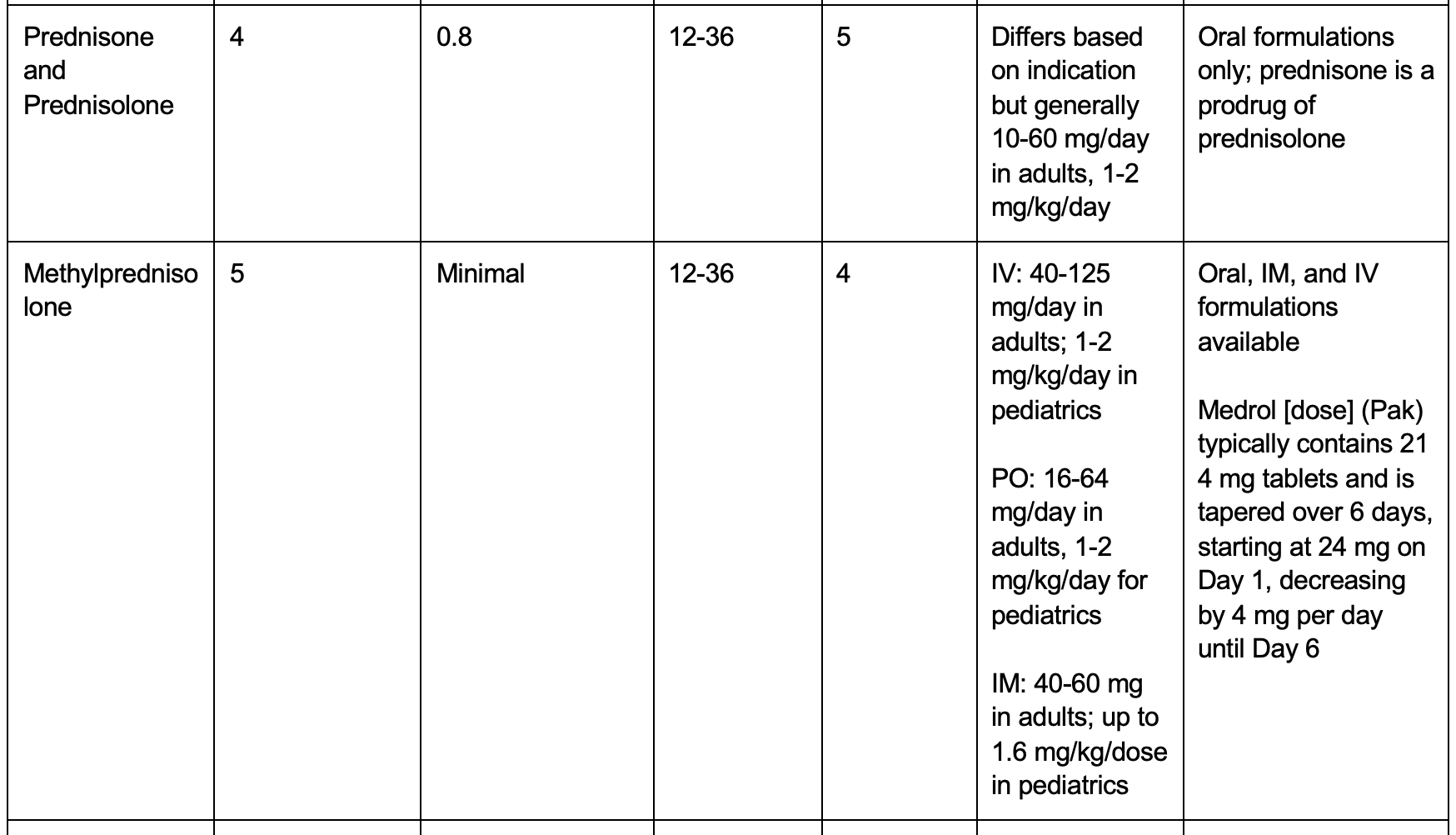
Table 1. Commonly used systemic steroids, with glucocorticoid and mineralocorticoid potencies relative to hydrocortisone.1-2 Abbreviations: IV – intravenous, PO – per os (oral), IM – intramuscular.


Agent Specifics
Hydrocortisone
Hydrocortisone is similar to the physiologic hormone, cortisol, and is classically the standard steroid to which glucocorticoid and mineralocorticoid potency is compared. Given its mineralocorticoid properties, hydrocortisone is traditionally used for adrenal insufficiency.1 Though hydrocortisone is often included in ‘crash carts,’ the most recent consensus on cardiopulmonary resuscitation (CPR) has a weak recommendation against the use of corticosteroids during CPR.6 However, due to the vasoconstrictive effects, hydrocortisone may be useful in refractory shock.7
Prednisone, Prednisolone, and Methylprednisolone
Both prednisone and prednisolone have similar effects on glucocorticoid and mineralocorticoid receptors.8 Prednisone is a prodrug and is converted in the liver to prednisolone.8 Subsequently, prednisolone is preferred in liver disease but is significantly more expensive than prednisone. Both prednisone and prednisolone are only available in oral formulations. Methylprednisolone is similar to prednisone and prednisolone but is available in oral, intramuscular, and intravenous formulations; however, please note the increased potency of glucocorticoid activity and negligible mineralocorticoid activity in methylprednisolone compared to prednisone or prednisolone.1
Dexamethasone
Dexamethasone is the strongest glucocorticoid among the commonly used steroids in the ED, with up to a 30 times potency compared to hydrocortisone and a 6-7 times potency compared to prednisone family.1 Dexamethasone is also the longest acting systemic steroid reviewed in this article. Due to both properties, dexamethasone can significantly suppress the hypothalamic-pituitary-adrenal (HPA) axis.1 However, due to its negligible effect on mineralocorticoid receptors, dexamethasone is useful in patients requiring an anti-inflammatory agent but are volume and sodium sensitive.1
Fludrocortisone
Fludrocortisone is also a prodrug that is activated in the liver.9 Given its potent mineralocorticoid effects, fludrocortisone is known to cause hypokalemia in up to 50% of patients, hypomagnesemia in up to 5% of patients, and severe hypertension.10 Heart failure, which appears to be volume dependent, can occur in up to 11% of patients.10 Despite being a systemic steroid and having anti-inflammatory properties, life-threatening hypersensitivity to fludrocortisone has been reported, though the mechanism is unknown.9
Adverse Effects
Adrenal insufficiency is a feared complication of prolonged corticosteroid use and abrupt cessation, with adrenal crisis as the most severe manifestation of insufficiency.11 This typically occurs due to suppression of the HPA axis. Symptoms may be vague, but hypoglycemia, hypotension, decreased exercise tolerance, and orthostasis in individuals with a history of prolonged steroid use should be evaluated for adrenal insufficiency.11 The duration considered prolonged is controversial, with as little as 5-days of high potency glucocorticoids causing adrenal suppression.1 However, in meta-analyses, there are no specific days or agents that reliably predict the development of adrenal insufficiency.12 Weight gain (up to 70%), development of cataracts (up to 15%), fractures (up to 12%), and neuropsychiatric events (up to 10%) are the most common adverse events.11 Furthermore, individuals with chronic steroid use should be considered at risk for new onset diabetes mellitus (OR 1.5-2.5) and cardiovascular disease (OR 1.2-2.56).11
Case Conclusion
After an hour of continuous nebulization treatment, the patient feels significantly improved with resolution of tachypnea, tachycardia, and hypoxia. You determine that the patient would benefit from the glucocorticoid properties of systemic steroids and prefer an agent with a longer duration due to his history of noncompliance. Subsequently, the patient receives dexamethasone. The patient is observed in the ED and discharged with follow-up in clinic the following week.
Take Home Points
- Not all steroids are created equally—consider their glucocorticoid and mineralocorticoid properties when selecting the optimal agent.
- Glucocorticoids provide the anti-inflammatory effects, and mineralocorticoids help retain sodium and fluid.
- Of the commonly used steroids in the ED, dexamethasone is the most potent glucocorticoid, and fludrocortisone is the most potent mineralocorticoid.
- Adrenal crisis is a rare but life-threatening manifestation of adrenal insufficiency that is precipitated by abrupt steroid cessation after chronic use.
- Consider the other complications of systemic steroids: weight gain, cataracts, fractures, and neuropsychiatric events.
References
1) Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. Published 2013 Aug 15.
2) Ericson-Neilsen W, Kaye AD. Steroids: pharmacology, complications, and practice delivery issues. Ochsner J. 2014;14(2):203-207.
3) Hodgens A, Sharman T. Corticosteroids. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 26, 2022.
4) Zennaro MC, Fernandes-Rosa F. 30 YEARS OF THE MINERALOCORTICOID RECEPTOR: Mineralocorticoid receptor mutations. J Endocrinol. 2017;234(1):T93-T106.
5) Te Riet L, van Esch JH, Roks AJ, van den Meiracker AH, Danser AH. Hypertension: renin-angiotensin-aldosterone system alterations. Circ Res. 2015;116(6):960-975.
6) Wyckoff MH, Greif R, Morley PT, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2022;146(25):e483-e557.
7) Gibbison B, López-López JA, Higgins JP, et al. Corticosteroids in septic shock: a systematic review and network meta-analysis. Crit Care. 2017;21(1):78. Published 2017 Mar 28.
8) Schijvens AM, Ter Heine R, de Wildt SN, Schreuder MF. Pharmacology and pharmacogenetics of prednisone and prednisolone in patients with nephrotic syndrome. Pediatr Nephrol. 2019;34(3):389-403.
9) Rahman M, Anjum F. Fludrocortisone. In: StatPearls. Treasure Island (FL): StatPearls Publishing; October 17, 2022.
10) Grijalva CG, Biaggioni I, Griffin MR, Shibao CA. Fludrocortisone Is Associated With a Higher Risk of All-Cause Hospitalizations Compared With Midodrine in Patients With Orthostatic Hypotension. J Am Heart Assoc. 2017;6(10):e006848. Published 2017 Oct 12.
11) Nicolaides NC, Pavlaki AN, Maria Alexandra MA, Chrousos GP. Glucocorticoid Therapy and Adrenal Suppression. In: Feingold KR, Anawalt B, Blackman MR, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; October 19, 2018.
12) Broersen LH, Pereira AM, Jørgensen JO, Dekkers OM. Adrenal Insufficiency in Corticosteroids Use: Systematic Review and Meta-Analysis. J Clin Endocrinol Metab. 2015;100(6):2171-2180.





2 thoughts on “Systemic Steroids: An ED Focused Overview”
Pingback: Nerdfallmedizin.de - Nerdwoche am 15.10.2023
Pingback: Week 39 – Endocrine – EM Ninja