Thrombocytopenia: An ED Approach
By Alex Koyfman MD and Elizabeth Brem MD
(Heme-Onc Fellow, Beth Israel Deaconess Medical Center)
Edited by Stephen Alerhand MD
Etiologies
1) Increased destruction
– Immunologic: collagen vascular disease, infection, ITP, lymphoma/CLL, drugs (heparin, sulfonamides, aspirin, phenytoin, digoxin, vancomycin, B-lactam antibiotics)
– Mechanical: TTP, HUS, DIC
– Vasculitis
2) Decreased production
– Decreased megakaryocytes: drugs (EtOH, thiazide, chemo, linezolid), toxins, infection, leukemia
– Splenic sequestration
3) Dilutional
– Massive transfusion, ECMO, exchange transfusion
Clinical presentation
– Petechiae, mucosal bleeding (epistaxis, gingival); spontaneous bleeding rare for platelets > 10, post-surgical bleeding rare if platelets > 50


Suggested work-up:
- Repeat platelet count – Ensure value is accurate
- CBC – TTP-HUS presents with anemia AND thrombocytopenia. Abnormal platelets and abnormal WBC count is concerning for primary hematologic etiology.
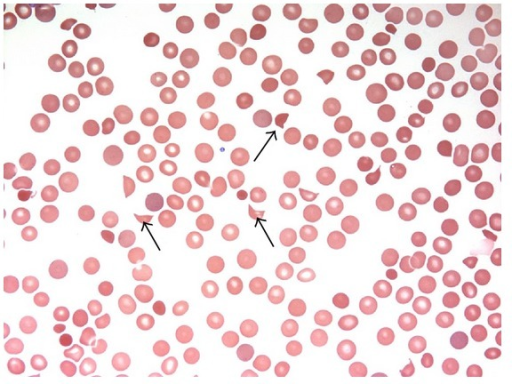
- Peripheral smear – Look for schistocytes, and also for platelet clumping to rule out pseudothrombocytopenia. If not comfortable looking at a smear yourself, call Hematology for help. Do not rely on automated instruments to rule in or out the presence of schistocytes.
- PT/PTT/INR/fibrinogen – These will be abnormal in DIC and unaffected in other etiologies.
- Physical exam: look for petechiae, hepatosplenomegaly

Whom to admit:
- Severe thrombocytopenia (i.e. < 20)
- Platelet count drop > 50% of baseline
- Suspected leukemia, TTP-HUS, or DIC
- Active bleeding
How to improve:
- Consider learning how to look at smears. It will be much easier to correctly dispo these patients if you can recognize pseudothrombocytopenia/platelet clumping and schistocytes.
- Check coags if platelets are low. DIC is a clinical diagnosis, and unlike with MAHA, there are no definitive findings on smear. If suspected, start work-up for underlying infectious cause.
Definitions and Learning Points:
HITT
– Heparin-induced thrombocytopenia AND thrombosis
– Use the 4T score: Timing (5-10 days after heparin exposure), degree of Thrombocytopenia (> 50% drop from baseline), no other clear etiology, and Thrombosis
– If intermediate probability, send anti-platelet (PF4) antibody test
– If high probability, start alternative anti-coagulation with argatroban (hepatically-cleared) or bivalirudin (renally-cleared)
ITP
– Dx of exclusion
– Acute => child, viral prodrome days-weeks prior, platelets <20, self-limited, supportive care unless active bleeding (steroids, IVIG, anti-Rh Ig)
– Chronic => adult, no prodrome, gradual, platelets 30-100
– Life-threatening bleeding: plt transfusions, steroids, IVIG
TTP-HUS
– Usually idiopathic but can be 2/2 meds (clopidogrel, ticlopidine, quinine) or infection (E. coli)
– Presume this is the Dx in anyone that presents with thrombocytopenia + microangiopathic hemolytic anemia (pentad of fever, anemia, thrombocytopenia, renal involvement, and neuro involvement [FAT RN] is rare, especially in adults).
– Acute management is with plasmapheresis. If your institution does not have this, start giving FFP and arrange for transfer to a tertiary care center. Do not give platelets, except perhaps in the case of acute hemorrhage (controversial).
Leukemia
– Typically presents with very high white counts, but sometimes can present with leukopenia, especially in the case of acute promyelocytic leukemia (APL). A low white count and DIC is concerning for APL, which is an Oncologic emergency
– Patients should be started on all-trans retinoid acid (ATRA) as soon as the diagnosis is suspected
– When to transfuse platelets: <10 or <50 + active bleeding or <50 + invasive procedure. Of note: transfused platelets last 3-5 days.
Further Reading
– Warkentin T. Heparin-Induced Thrombocytopenia: Diagnosis and Management. Circulation 2004;110:e454-e8. http://circ.ahajournals.org/content/110/18/e454.full
– http://www.ncbi.nlm.nih.gov/pubmed/25060257
– http://www.ncbi.nlm.nih.gov/pubmed/25060255
– http://www.ncbi.nlm.nih.gov/pubmed/22445678
– http://www.ncbi.nlm.nih.gov/pubmed/17961957







1 thought on “Thrombocytopenia: An ED Approach”
Pingback: Thrombocytopenia – EM Clerkship