Authors: Lucas Goss, MD (EM Resident Physician, Carolinas Medical Center, Charlotte, NC) and Kathryn T Kopec, DO (@KopecToxEM, EM Attending Physician, Medical Toxicologist, Carolinas Medical Center, Charlotte, NC) // Reviewed by: James Dazhe Cao, MD (@JamesCaoMD, Associate Professor of EM, Medical Toxicology, UT Southwestern Medical Center, Dallas, TX); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)

Case:
A 50-year-old male presented to the emergency department for cough, fever, and shortness of breath. He had a history of traumatic brain injury and spinal cord injury with subsequent lower extremity paralysis secondary to a motor vehicle accident four months ago. Initial vital signs were blood pressure 96/54 mmHg, heart rate 118 beats per minute, O2 sat 88% on non-rebreather facemask, respiratory rate 30 breaths/minute and temperature of 102.4F. His chest x-ray demonstrated a right sided pneumonia and laboratory findings included lactate 4 mmol/L, K+ 4.2 mmol/L, Creatinine 1.5 mg/dL, BUN 38 mg/dL, and glucose 130 mg/dL. The patient’s respiratory status worsened, and he was emergently intubated with 1.5 mg/kg of ketamine and 1 mg/kg of succinylcholine. Approximately three minutes after administering rapid sequence intubation drugs the patient went into a wide complex bradycardia that quickly degenerated into ventricular fibrillation.
Questions:
- What is the mechanisms of action of the depolarizing neuromuscular blocker (NMB) succinylcholine?
- What are the adverse effects of neuromuscular blocking agents?
- What is the mechanism of succinylcholine induced hyperkalemia, and how do we identify those at risk?
- What is the mechanism of action of non-depolarizing neuromuscular blockade?
- How are non-depolarizing NMBs (i.e., rocuronium) different from depolarizing agents, and why do they not pose the same risk of hyperkalemia?
- Why is succinylcholine contraindicated in this case?
Depolarizing Neuromuscular Blockade – Succinylcholine:
- Mechanism:
- Succinylcholine is an analog of acetylcholine (ACh). In healthy patients, it binds ACh receptors at the neuromuscular junction (NMJ) causing depolarization of the cell membrane which results in muscular fasciculations.1 The fasciculations are secondary to the sustained endplate depolarization causing the Na+ channels to remain in the inactive state for a prolonged period. When the cell membrane is depolarized, sodium flows inward, and potassium flows out of the cell.1
- Adverse Effect:
- This flow of potassium to the extracellular space can come at a cost. In normal individuals 1 mg/kg of succinylcholine causes serum [K+] to increase by approximately 0.5 mEq/L.1 This raises the concern for succinylcholine’s use in patients who are at risk for hyperkalemia.
What is the mechanism of succinylcholine induced hyperkalemia, and how do we identify those at risk?
Healthy patients have a normal amount of ACh receptors primarily concentrated at the NMJ. Succinylcholine is given and normal muscle contraction occurs with ACh released at the NMJ. Acetylcholine is then quickly broken down by acetylcholinesterases.1,2 However, when someone has loss of consistent muscle contractions, such as a paraplegic or quadriplegic patient, there is an upregulation and expression of ACh receptors. This means that there are more potential receptors for succinylcholine to bind. These receptors are not only increased in amount but also spread across the entire muscle membrane instead of being concentrated at the NMJ.2 In normal muscle contractions, ACh is only released locally at the NMJ. However, when succinylcholine is administered in a patient with upregulated ACh receptors, it is able to reach outside of the NMJ as well.
Additionally in conditions like burns, sepsis, upper motor neuron disease, or lower motor neuron disease, proliferation of immature ACh receptors occurs. These receptors cause more efflux of potassium when bound compared to mature ACh receptors.3,4,5 This, in combination with the increased total amount of available receptors to bind, can cause a massive release of potassium. In addition, succinylcholine is not efficiently broken down by traditional acetylcholinesterases, so it sticks around much longer.1 These effects can result in severe hyperkalemia causing cardiac arrest, as what happened in our case above.
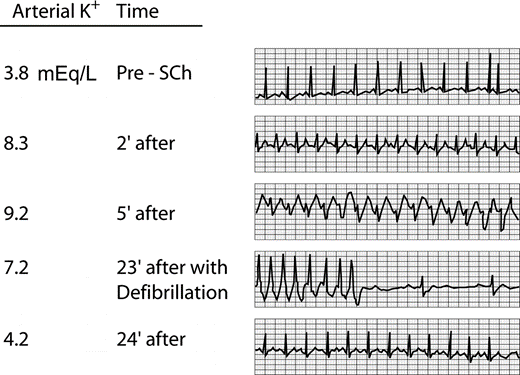
The effect of succinylcholine induced hyperkalemia has been demonstrated to occur as far back as 1969 when Mazze et al. examined potassium levels before and after succinylcholine in 16 patients who recently experienced orthopedic trauma with massive wounds.6 The figure below from Mazze et al. demonstrates the changes in potassium and EKG effects over time after the administration of succinylcholine in one of the patients in the study.6
Plane et al. described another case in a patient that was intubated in the ICU for 31 days for respiratory distress. Upon extubating the patient had respiratory distress requiring re-intubation. The patient’s potassium prior to re-intubation was 3.5 mmol/L. The patient was intubated using 1 mg/kg of succinylcholine, and shortly after had a cardiac arrest with progressive ECG changes that evolved from normal, to peaked T waves, widened QRS, and a sine wave pattern. Repeat potassium level after intubation was 9.6 mmol/L.7
The main learning point is anything that causes functional denervation (critical illness myopathy), anatomical denervation (chronic ischemia, end-stage renal disease, diabetes mellitus, Guillain Barre Syndrome, myasthenia gravis, stroke), prolonged immobilization, or burns can increase the risk of succinylcholine induced hyperkalemia. In our case, the patient had multiple risk factors for succinylcholine induced hyperkalemia (prolonged immobilization and denervation) from his recent trauma.
Non-Depolarizing Neuromuscular Blockade:
Non-depolarizing neuromuscular blockers are classified by structure into two categories although they all exhibit the same mechanism of action. These two categories differ in their adverse effects, as well as their ability to be reversed.
- Categories of non-depolarizing neuromuscular blockers
- Aminosteroidal:
- Pancuronium, rocuronium, vecuronium
- Benzylisoquinolinium:
- Atracurium, cisatracurium, mivacurium
- Aminosteroidal:
- Mechanism of action:
- Non-depolarizing agents act via competitive inhibition, blocking ACh from binding
- Adverse effects of non-depolarizing neuromuscular blocking agents:
- The most common adverse effect of non-depolarizing NMBs is non-IgE mediated histamine release.1 This can cause tachycardia, hypotension, bronchospasm, and urticaria.
- The use of vecuronium and rocuronium for more prolonged infusions, especially when combined with steroids (i.e., severe COVID-19 treatment), can result in prolonged profound weakness.9 Instead use of a benzylisoquinolinium, such as cisatracurium, may be used to prevent this adverse effect.
- Atracurium and cisatracurium are metabolized and produce a metabolite called laudanosine. In cases of hepatic failure and prolonged infusions, this metabolite can build up and potentially precipitate seizures,10,11 however this is not well described clinically.12
Why does hyperkalemia not occur with non-depolarizing neuromuscular blocking agents?
Remember that succinylcholine is what is called a depolarizing NMB agent. Non-depolarizing means it does not cause an action potential. During normal muscle contractions, ACh is released from the presynaptic terminal, diffuses across the synaptic membrane, and binds nicotinic ACh receptors on the motor end-plate.1,8 This causes activation of sodium channels and causes influx of sodium which depolarizes the cell. When this happens potassium channels also open that cause efflux of potassium. Depolarization causes intracellular calcium release which ultimately results in muscular contractions.8,9
Instead, non-depolarizing agents act via competitive inhibition, blocking ACh from binding.1 Since, they do not cause depolarization of the cell there is no associated potassium release. Although non-depolarizing agents have the advantage of not causing hyperkalemia, they are not without adverse effects.
Another difference between depolarizing and non-depolarizing NMBs is that non-depolarizing NMBs have the potential to be reversed by increasing the amount of acetylcholine available to bind at the NMJ. This explains why cholinesterase inhibitors, such as neostigmine, can be used to reverse non-depolarizing neuromuscular blockade. Neostigmine is used in combination with glycopyrrolate, an anti-muscarinic agent, to avoid excessive muscarinic stimulation that would otherwise have the potential to cause bronchospasm and laryngeal collapse.11 This combination is typically used for reversal of aminosteroidal NMBs.
Another reversal agent, sugammadex, is a non-depolarizing NMB binding agent that preferentially binds and reverse the actions of steroidal NMBs such as vecuronium or rocuronium.11
Case Follow-up:
Fortunately, the providers in this case were astute enough to recognize the wide complex rhythm and potential for succinylcholine induced hyperkalemia. Two grams of calcium chloride were given, and two round of compressions were performed with subsequent ROSC. A VBG was sent and demonstrated a potassium of 7.2. The patient was temporized and transferred to the ICU, where their hyperkalemia resolved.
Clinical Pearls:
- Any condition that causes prolonged immobilization, denervation, or significant myopathy can predispose patients to succinylcholine-induced hyperkalemia
- Succinylcholine-induced fasciculations occur because of prolonged depolarization from ACh
- Non-depolarizing NMBs work through competitive inhibition and do not cause potassium release or muscle contractions
- Non-depolarizing NMBs may cause non-IgE mediated histamine release
- Aminosteroidal non-depolarizing NMBs have the potential to be reversed by cholinesterase inhibitors and/or sugammadex
References:
- Guo CJ, Sutin KM. Neuromuscular Blockers. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds. Goldfrank’s Toxicologic Emergencies, 11e. McGraw Hill; Accessed August 15, 2021.
- Martyn JA, Richtsfeld M. Succinylcholine-induced hyperkalemia in acquired pathologic states: etiologic factors and molecular mechanisms. Anesthesiology. 2006 Jan;104(1):158-69. doi: 10.1097/00000542-200601000-00022.
- Fischer U, Reinhardt S, Albuquerque EX, Maelicke A. Expression of functional alpha7 nicotinic acetylcholine receptor during mammalian muscle development and denervation. Eur J Neurosci. 1999 Aug;11(8):2856-64. doi: 10.1046/j.1460-9568.1999.00703.x.
- Tsuneki H, Salas R, Dani JA. Mouse muscle denervation increases expression of an alpha7 nicotinic receptor with unusual pharmacology. J Physiol. 2003 Feb 15;547(Pt 1):169-79. doi: 10.1113/jphysiol.2002.036368. Epub 2002 Dec 20.
- Adeyinka A, Layer DA. Neuromuscular Blocking Agents. 2021 Dec 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537168/
- Mazze RI, Escue HM, Houston JB. Hyperkalemia and cardiovascular collapse following administration of succinylcholine to the traumatized patient. Anesthesiology. 1969 Dec;31(6):540-7. doi: 10.1097/00000542-196912000-00006.
- Plane AF, Marsan PE, du Cheyron D, Valette X. Rapidly changing ECG in hyperkalaemia after succinylcholine. Lancet. 2019;393(10184):1983. doi:10.1016/S0140-6736(19)30838-4
- Gash MC, Kandle PF, Murray I, Varacallo M. Physiology, Muscle Contraction. 2021 Apr 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537140/
- Murray MJ, Brull SJ, Bolton CF. Brief review: Nondepolarizing neuromuscular blocking drugs and critical illness myopathy. Can J Anaesth. 2006 Nov;53(11):1148-56. doi: 10.1007/BF03022883.
- Sakuraba S, Hosokawa Y, Kaku Y, Takeda J, Kuwana S. Laudanosine has no effects on respiratory activity but induces non-respiratory excitement activity in isolated brainstem-spinal cord preparation of neonatal rats. Adv Exp Med Biol. 2010;669:177-80. doi: 10.1007/978-1-4419-5692-7_35.
- Clar DT, Liu M. Non-depolarizing Neuromuscular Blockers. 2021 Dec 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534828/
- Fodale V, Santamaria LB. Laudanosine, an atracurium and cisatracurium metabolite. Eur J Anaesthesiol. 2002 Jul;19(7):466-73. doi: 10.1017/s0265021502000777.






