
Author: Cynthia Santos, MD (Senior Medical Toxicology Fellow, Emory University School of Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
Case Presentation:
A 45 year old male presents intoxicated, smelling of alcohol and appears disheveled with vomit on his clothes. He is sleepy but arousable to noxious stimuli. His serum ethanol level is 143 mg/dL. Na 135, K 3.9, Cl 97, CO2 20, BUN 33, Cr 1.1. Lactate 3.1. pH 7.35, CO2 28, HCO3 15. His urine is negative for ketones. His vitals are HR 103, RR 30, BP 115/65, O2 98% RA.
Question:
Could these laboratory results be consistent with alcohol ketoacidosis (AKA)?
Pearl:
The classic laboratory findings in patients with AKA include an elevated anion gap metabolic acidosis and an elevated lactate. Early in AKA patients may be negative for ketones when the nitroprusside test is used because it does not detect beta-hydroxybutyrate. As patients recover, the nitroprusside test will become positive as beta-hydroxybutyrate gets converted to acetone and acetate.
Acid/base status:
- Patients with AKA typically have elevated anion gap metabolic acidosis. However, vomiting may cause a primary metabolic alkalosis and a compensatory respiratory alkalosis which may result in a normal or even elevated pH.
- AKA patients, as compared to DKA patients, typically have higher pH, lower K and Cl, and higher HCO3 in their blood tests.
High Redox State (Excess NADH):
- As ethanol is metabolized by ADH and ALDH to acetaldehyde and acetate, respectively, an increased amount of NADH forms which causes a high redox state and excess of reducing potential (increased NADH:NAD+ ratio).

Increased lactate due to pyruvate shunting:
- Reduced caloric intake, decreased glycogen stores, and thiamine depletion results in amino acids being converted to pyruvate. The excess pyruvate that forms can then be diverted to gluconeogenesis, be converted to acetyl-CoA, which can enter the Kreb’s cycle, or can enter various biosynthetic pathways (e.g. fatty acids, ketones, etc.). Pyruvate can be diverted to these pathways if there is sufficient NAD+.
- However ethanol causes a high redox state (excess NADH). In the setting of a high redox state ethanol results in increased lactate due to the conversion of pyruvate to lactate and diverts pyruvate from gluconeogenesis.

Figure source: Shull P, & Rapoport J.
Anion gap primarily due to beta-hydroxybutyrate:
- The primary anion contributor in patients with AKA and diabetic ketoacidosis (DKA) is beta-hydroxybutyrate with lactate having less of a role.
- Decreased caloric intake and glycogen stores results in increased fatty acid mobilization and oxidation resulting in increased acetyl-CoA. In normal states (when there is sufficient NAD+) acetyl-CoA can then enter the Kreb’s cycle or be used in fatty acid synthesis. Thiamine also facilitates the entry of acetyl-CoA into the Kreb’s cycle.
- However, when there is a high redox state (excess NADH) and thiamine deficiency acetyl-CoA gets converted to acetoacetate which then gets converted to beta-hydroxybutyrate.
Ketone production:
- Early the main anion contributor is beta-hydroxybutyrate, which is not detected well by the nitroprusside test (used to detect ketones in serum and urine). The nitroprusside test does not detect beta-hydroxybutyrate, although it is good for detecting acetoacetate and acetone.
- It is common for early AKA to have a falsely negative ketone test if the nitroprusside test is used because of the test’s inability to detect beta-hydroxybutyrate. If available, specific assays for beta-hydroxybutyrate should be done.
- As patients recover and receive glucose and thiamine supplementation, ATP is made which reverses the pyruvate-to- lactate and NAD+-to-NADH ratios. This allows beta-hydroxybutyrate to be converted to acetoacetate and as patients recover the nitroprusside test will actually become more positive due to the increased production of acetoacetate.
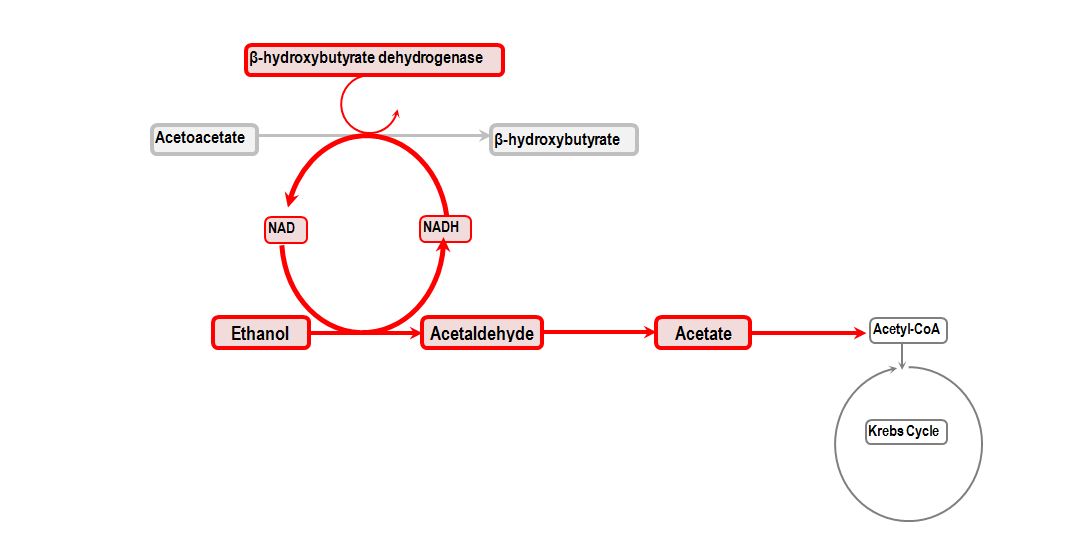
Figure Source: www.derangedphysiology.com
Main Point:
The classic laboratory findings in patients with AKA include an elevated anion gap metabolic acidosis, and elevated lactate that is insufficient to account for the gap. The main anion contributor early in AKA is beta-hydroxybutyrate, but it will not be detected when evaluating for ketones using the nitroprusside test. As patients recover and are given glucose and thiamine supplementation, the lactate will decrease as pyruvate is no longer shunted to lactate and instead enters the Kreb’s cycle and other biosynthetic pathways. The anion gap decreases as beta-hydroxybutyrate gets converted to acetone and acetate. The nitroprusside test then becomes positive for ketones later as patients recover.
Resources:
- Yip L. Ethanol, Chapter in Goldfrank’s Toxicological Emergencies. Tenth Edition. Editors: Hoffman R, Howland M, Lewin N, Nelson L, Goldfrank L. McGraw Hill (2015); New York.
- Woods W, Perrina D. Alcohol Ketoacidosis, Chapter in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th Edition. Editors: Tintinalli JE, et al. McGraw Hill (2011); New York.
- Shull P, & Rapoport J. Life-threatening reversible acidosis caused by alcohol abuse. Nature Reviews Nephrology (2010) 6, 555-559
- Diabetic, Alcoholic, and Starvation Ketoacidosis. Chapter 6.17. Available at: http://www.derangedphysiology.com/main/core-topics-intensive-care/acid-base-disturbances/Chapter%206.1.7/diabetic-alcoholic-and-starvation-ketoacidosis







2 thoughts on “Toxcards: Alcoholic Ketoacidosis”
Pingback: emDOCs.net – Emergency Medicine EducationThe EM Educator Series: Why did the patient with alcohol dependence stop drinking? - emDOCs.net - Emergency Medicine Education
Pingback: Alkoholketoacidos – Mind palace of an ER doc