Originally published on Ultrasound G.E.L. on 4/26/21 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!
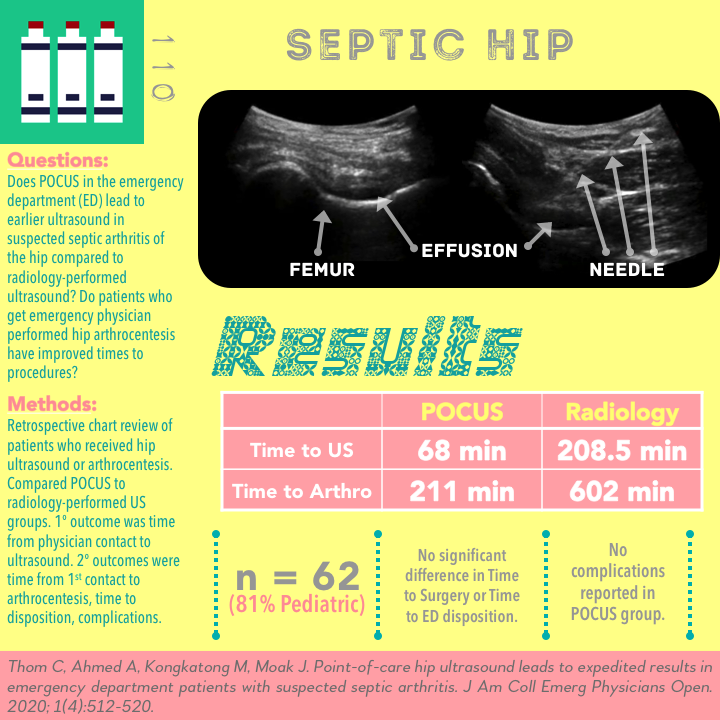
Point-of-care hip ultrasound leads to expedited results in emergency department patients with suspected septic arthritis
J Am Coll Emerg Physicians Open June 2020 – Pub Med Link
Unrelated Cases Mentioned in Podcast
Take Home Points
1. This small retrospective study demonstrates potential benefits of emergency physician performed hip ultrasound and arthrocentesis in saving time to diagnosis in the work up of septic arthritis.
2. Even putting aside the study limitations, it remains unclear if this degree of time savings would have significant impact on patient centered outcomes.
3. Prospective, larger studies would be valuable in assessing both clinician centered (time to disposition) and patient centered (function, morbidity, mortality) outcomes.
Background
Ultrasound has proven itself useful in identifying hip effusions, especially in pediatric patients. More recently it has been used to guide hip joint aspirations, such as in the case of suspected septic arthritis. Because of the complex anatomy and lack of training in the procedure, many providers are reluctant to blindly stick a needle into the hip. Ultrasound-guidance has the potential to make this safer. In many cases, delaying the arthrocentesis can lead to delays in patient care; this can unfortunately occur if waiting for consulting services to perform this procedure. Therefore, POCUS offers a potential opportunity to improve patient care not just by expediting the diagnosis of an effusion but by also expediting the arthrocentesis. In this article, the authors put this idea to the test. They studied patients with suspected septic arthritis of the hip, comparing a POCUS group to a radiology-performed ultrasound group for outcomes of times to diagnosis and management.
Questions
Do patients with suspected septic arthritis of the hip who were evaluated with point of care ultrasound have faster times to ultrasound compared to those who have an ultrasound from the radiology department?
Do those patients who receive hip arthrocentesis by the treating emergency physician have differences in time to procedure?
Population
Emergency department patients, 2016 to 2019
Inclusion:
- All patient who received a hip ultrasound or hip arthrocentesis in the ED
- They found these patients by reviewing the interpretation of every single ultrasound study done in this time period.
Exclusion:
- History of prior hip surgery
- History of prior hip infection
- Trauma
- Transferred with known diagnosis of septic arthritis
Design
Retrospective single academic center
Searched for patients that meet inclusion criteria.
They also searched the electronic health record by ICD-10 code for anyone that could have had an arthrocentesis.
Recorded all the times:
- Time from first emergency physician (EP) contact to time of ultrasound (for radiology performed ultrasound they used the time to the interpretation by radiology, for emergency performed they used the time the first image was saved).
- Time from first EP contact to time of needle entry into joint space.
- Time from patient arrival to ED disposition
- Time from ED physician contact to OR start.
Primary outcome – time from first EP patient contact to ultrasound, comparing POCUS group to Radiology-performed ultrasound group
Secondary outcomes – Time from first EP contact to arthrocentesis, time to disposition, complications following EP performed arthrocentesis.
Who did the ultrasounds?
Scheduled annual didactics on hip sonography and arthrocentesis + hands on teaching in cadaver lab
10 different resident physicians and 9 different supervising attendings did the scans.
The Scan
Linear or Curvilinear


Visualize femoral neck in long axis, looking for effusion
Compare to contralateral hip
Positive = effusion ≥5 mm (from femoral neck) or if >2 mm greater than asymptomatic side
Learn how to do Hip Ultrasound from 5 Minute Sono!

Check out Hip Pathology on the POCUS Atlas!

Highland Ultrasound – US Guided Hip Arthrocentesis
Results
N = 62
- 74 met inclusion, 12 were excluded based on criteria
- 17.7% of patients were adults
- 22/62 (35.5%) EP hip POCUS, 10/22(45.5%) had EP arthrocentesis
- 36/62 (58.1%) had radiology ultrasound, 3/36 (8.3%) had radiology performed arthrocentesis
- 4 patients had no ultrasound but had a radiology performed arthrocentesis
- No significant differences between POCUS and radiology US groups in terms of age, % of septic arthritis, Kocher criteria, ability to ambulate, admission, OR intervention
Primary Outcome – Median Time from EP contact to Ultrasound
EP POCUS group (n=22) 68 minutes (IQR 38.8-132)
Radiology performed group (n = 36) 208.5 minutes (IQR 163.8-301.3).
Difference of 140.5 minutes (2.34 hours)
Secondary Outcomes
Median Time from EP contact to arthrocentesis
EP performed (n = 10) 211 minutes (IQR 141.3-321.5)
Radiology performed (n = 7) 602 minutes (IQR 500-692)
Difference of 391 minutes (6.52 hours)
No reported complications in the EP group. 100% success.
✱ Note: Not statistically significant but some indications that the radiology performed arthrocentesis group might have been sicker than the EP performed arthrocentesis group (100% admission vs 60%, 86% OR intervention vs 60%, 0% ambulatory vs 40%)
Median Time from ED arrival to OR start
- EP performed arthrocentesis 586 minutes (IQR 448-1032)
- Radiology performed arthrocentesis 1019 minutes (IQR 595-1614)
- Not statistically significant. Difference of 433 minutes (7.22 hours)
Median Time from ED arrival to ED disposition
- EP performed hip ultrasound 313 minutes (IQR 268-502)
- Radiology performed ultrasound 407 minutes (IQR 288-583)
- Not statistically significant. Difference of 94 minutes.
The longest wait for a radiology performed ultrasound result was nearly 15 hours! Hopefully that was a case in which it was ordered late.
Strengths
Very little prior evidence on this topic. This is the largest series of patients for this research question.
Went beyond accuracy to measure impacts in management times
Limitations
Retrospective. There is a lot of potential for confounding in the times measured. As the authors bring up – what determined when the EP decided to do the ultrasound or arthrocentesis? In addition, maybe those physicians were different from “standard” emergency physicians. Perhaps the EP did not do an ultrasound or procedure when it was thought to be difficult, that would really bias the comparison if the EP’s did the easy ones and radiology did all of the difficult ones.
Small sample size overall and very limited number of patients who received arthrocentesis. The study was not powered to show complications between groups so that must be kept in mind going forward (see next point below).
Fairly high amount of training in hip arthrocentesis compared to many centers. This limits the external validity. If the operators were less experienced it could lead to delays (such as from failed attempts) and perhaps a less robust difference in time outcomes. The accuracy of the hip ultrasound was not assessed here. It seemed to be assumed that the ED providers were accurate at diagnosing hip effusions, which may not be the case for everyone. The same goes for complications from performing an arthrocentesis. This study showed no complications from ED performed arthrocentesis, but that is only based on 10 patients! This means that if an important complication occurred 1 in 20 times (this is just a made up number), you might not see evidence of that in this study. Complications could be even more frequent if the procedure was performed by providers with less comfort and training in this application. It is not necessarily true that this study underrepresents the harms, but the point is that we just can’t say based on this data.
Discussion
For the primary outcome of Time to Ultrasound the study design was such that it favored the POCUS group. This is because for the POCUS group they compared the Time to first EP performed ultrasound (the time on the first saved clip) versus in the radiology group the clock stopped only after there was a radiologist’s interpretation. Although somewhat unfair, this is actually a common way to make this comparison in POCUS studies. The authors acknowledge this and felt this most closely resembled actual practice. I tend to agree with that. Part of the benefit of POCUS is that the image acquisition and interpretation is happening simultaneously at the bedside. Just realize that if the EP looked at the radiology-performed images once they were available, perhaps that could cut down on the time difference as well.
Patient centered outcomes? A lower time to diagnosis and intervention seems like a great idea, but do we know if it directly translates to a patient’s outcome from this disease? We have all been taught that the longer someone has septic arthritis, the more likely joint damage can occur. Although it makes sense intuitively that it would be better to get these patients to a therapeutic intervention, we don’t know if the time differences seen between these groups (on the scale of hours) would have a significant clinical impact. In fact, despite the earlier arthrocentesis in the POCUS group, there was not a statistically significant difference in the time to the operating room. Therefore, it is still unclear if this will significantly impact the patient’s ultimate outcomes. Theoretically, early diagnosis could allow for earlier antibiotics which could make a difference? We should keep in mind that a larger study might in fact show these differences to be significant. In this study, the POCUS group got to the operating room an average of 7 hours before the radiology group – it just was not statistically significant.
Summary
This a retrospective chart review study of 62 ED patients undergoing a hip ultrasound. Based on their median times, the group receiving POCUS by the EP had an ultrasound over 2 hours earlier than those receiving radiology ultrasound. For the subset who received arthrocentesis, there was a savings of 6.5 hours if it was performed by the EP instead of radiology.
Take Home Points
1. This small retrospective study demonstrates potential benefits of emergency physician performed hip ultrasound and arthrocentesis in saving time to diagnosis in the work up of septic arthritis.
2. Even putting aside the study limitations, it remains unclear if this degree of time savings would have significant impact on patient centered outcomes.
3. Prospective, larger studies would be valuable in assessing both clinician centered (time to disposition) and patient centered (function, morbidity, mortality) outcomes.
More Great FOAMed on This Topic
EM DOCS – Hip Ultrasound and Arthrocentesis
Core EM – Pediatric Septic Hip
Our score

Expert Reviewer for this Post

J. Matthew Fields, MD FACEP @jmatthewfields
Research Director, Health Design Lab; Affiliate Faculty, Thomas Jefferson Emergency Ultrasound; Associate Professor, Dept of Emergency Medicine; Sidney Kimmel Medical College + Thomas Jefferson University Hospitals
Reviewer’s Comments
I agree with the consensus of the review. For a retrospective study, the authors did a nice job of pulling out multiple data points that enable the reader to reach some conclusions. The study confirms what we often observe in real practice, that when EPs are trained and equipped with POCUS they can rapidly perform hip ultrasound and diagnose an effusion. It stands to reason that this time reduction would at some threshold translate to a meaningful improvement in outcomes, but this requires more study.
Cite this post as
Michael Prats. Septic Arthritis of the Hip. Ultrasound G.E.L. Podcast Blog. Published on April 26, 2021. Accessed on October 1, 2021. Available at https://www.ultrasoundgel.org/110.






