Authors: Gurpreet Kaur, DO (@KaurGurpreetDO, EM Resident, University of Kentucky, Lexington, KY), Aaron C. Tyagi, MD (Assistant Professor of Emergency & Critical Care Medicine, University of Kentucky, Lexington, KY) // Reviewed by: Michael Yoo, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Cases
#1: A 50-year-old woman presents to the emergency department (ED) with generalized weakness and epigastric pain. Review of systems (ROS) is positive for one episode of dark tarry stools. The patient frequently takes naproxen for her arthritis, but her past medical history is otherwise unremarkable. Vital signs are notable for: HR 80 bpm, BP 120/66 mmHg, RR 20, saturating 98% on RA. Her physical exam demonstrates mild tenderness in the epigastrium, and a rectal exam is positive for melena.
#2: A 45-year-old woman presents to the ED with a chief complaint of hematemesis. She had one episode of coffee ground emesis at home prior to arrival with continued nausea. ROS is negative for abdominal pain, diarrhea, blood in stool, or dark tarry stools. However, the patient endorses daily consumption of alcohol. Her initial vital signs are HR 110 bpm, BP 105/64 mmHg, RR 25, saturating on 98% RA. Physical exam is notable for intact mentation, jaundice, and a soft but distended abdomen with spider angiomas with diffuse tenderness. While being examined, the patient starts to have emesis with bright red blood.
What are the first steps to taking care of both patients? What are the dispositions of these patients? What will help determine the disposition?
Introduction
Acute upper GI bleeding (UGIB) is defined as bleeding from a source proximal to the ligament of Treitz. UGIBs are associated with significant morbidity and mortality and can be a true GI emergency.1 Acute UGIBs can be divided into non-variceal and variceal etiologies. Non-variceal UGIBs are the most common type of acute UGIB and includes peptic ulcer disease, gastroduodenal erosions, Mallory-Weiss tears, erosive esophagitis, arterio-venous malformations, Dieulafoy lesions, tumors, and malignancies.2
Peptic ulcers are most commonly caused by a Helicobacter pylori (H. pylori) infection or use of non-steroidal anti-inflammatory drugs (NSAID) or anti-platelet medications such as aspirin.3 Variceal bleeds are the third most common cause of UGIB and should be considered in a patient with a history of cirrhosis or chronic alcohol abuse.2,4 The severity of the underlying cirrhosis is directly related to the probability of a patient having varicies.5 Physical exam findings which may help identify patients with chronic liver disease with exacerbation or undiagnosed liver disease include ascites, caput medusae, or spider angiomas.4
Presentations for UGIB can range from asymptomatic to melena with or without coffee ground emesis to massive life-threatening hemorrhage.2 Subsequently, the ultimate disposition ranges from discharge with close follow-up for stable patients to ICU admission. This article aims to answer the following questions: what factors determine the level of care of UGIB patients, and what can emergency medicine providers use to risk stratify patients with acute UGIB?
Evaluation
As with every patient, start with the ABCs. This involves making sure that the patient is protecting their airway in the setting of bloody emesis, breathing, and evaluating for impending circulatory compromise.1 Obtaining two large bore IVs (ideally 18 gauge or larger) in every UGIB patient is ideal, one for giving blood products and the other for medications.
After patient stabilization, obtaining a thorough history including the onset, duration, and intensity of symptoms will help identify the etiology of UGIB. This includes asking about prior episodes, known lesions or ulcers, and prior interventions.1 Past medical history including cirrhosis, chronic NSAID use, antiplatelet agents, anticoagulants, or steroid use will assist with risk stratification.1,4 If the patient is unable to provide history, attempt to obtain collateral information from family members, guardians, care takers, or the sending facility.
Always obtain and reassess vital signs as tachycardia or tachypnea despite hemodynamic stability may be the first indicators of active or significant bleeding.5 Delayed capillary refill time and conjunctival pallor may also be clues of acute blood loss anemia. A complete abdominal exam and rectal exam should be performed to assess for tenderness to palpation, peritoneal signs, presence of melena, or bright red blood in the rectal vault.1,4
The use of fecal occult blood testing (FOBT) in assessing patients with suspected GI bleed is controversial. FOBT is only validated as a screening tool for colorectal cancer and has very poor sensitivity for active GI bleeding, with many false negatives and positives.6-8 Clinical judgements made based on FOBT have resulted in adverse care including inappropriate endoscopy and missed malignancies.6-7 Sharma et al. preformed a retrospective chart review of 1000 patients and noted that only 17% of patients with a positive FOBT had active GI bleeding.7 The authors concluded that the test is inappropriate for evaluating for acute GI bleeding and should be preferentially used as a colorectal cancer screening.7 Several institutions have removed FOBT in the ED or the entire hospital.8
Lab work should include a complete blood count, comprehensive metabolic panel, type and cross, and coagulation panel.1Troponins and EKGs may further identify demand ischemia.1 We emphasize that patients with acute massive bleed can have normal hemoglobin levels due to the delayed nature of hemoglobin measuring.1 The BUN/Cr ratio can help differentiate between UGIB or LGIB; BUN/Cr > 30 suggests UGIB.9
Management
Resuscitation of patients with an acute UGIB starts with addressing hemodynamic stability with cautious fluid resuscitation and blood transfusions in patients with Hb <7 or ongoing bleeding.4,20-22 Any coagulopathy should be corrected, and anticoagulation should be reversed.4 Endotracheal intubation should be considered on patients with high risk for aspiration in cases of ongoing hematemesis or altered mental status.1,4,20,22 Medical therapies include giving the patients a proton pump inhibitor (PPI), antibiotics, and prokinetic agents.4,12 An 80 mg bolus followed by an 8 mg/h infusion of pantoprazole for 72 hours is recommended by the current American College of Gastroenterology (ACG)guidelines. Intermittent dosing of 40 mg PO/IV BID has shown noninferiority and can be considered. Octreotide (50 mcg bolus, followed by a continuous infusion of 50 mcg/hour) can be considered in patients with acute variceal bleeding.13 While there is not robust evidence that octreotide affects mortality, it may improve the efficacy of endoscopic therapy.4,14Patients with cirrhosis or liver disease should be given third-generation cephalosporin antibiotics (Ceftriaxone 1 g once daily for a total duration of 7 days) which is associated with improved survival.4,15 However, always consider broadening antibiotic therapy in cases of presumed concomitant sepsis. Prokinetics such as erythromycin (250 mg or 3 mg/kg given over 5 to 30 min) or metoclopramide (20 mg IV) can be considered prior to endoscopy to improve visualization, in conjunction with GI specialists.4,12 Endoscopic therapy is used as both diagnostic and therapeutic for UGIB patients.
As mentioned above, patients with UGIB may require intubation for altered mental status or ongoing hematemesis. Unlike massive hemoptysis, there is no clear quantification for massive hematemesis. Intubating a patient with active massive hematemesis can be very difficult due to active hemorrhage obscuring the view of the vocal cords, increased risk of aspiration, and hemodynamic instability. EMCrit and Life in the Fastlane have great posts on the approach to intubating a patient with an UGIB.16,17 We briefly review some key points below.
Intubating a UGIB patient16- 18
- Ensure appropriate PPE with gloves, gown, mask, and eye protection.
- Ensure multiple suction sources. Backup airway devices such as bougie, adjunct airways, direct laryngoscopes should be readily available.
- Optimize hemodynamics by resuscitating the patient first. This can include transfusing the patient, activating MTP, or starting vasopressors if needed.
- Consider emptying the stomach by either using prokinetics drugs such as metoclopramide or erythromycin or inserting a large bore nasogastric tube. Choose an induction agent that is hemodynamically neutral, if available, such as ketamine or etomidate.
- Preoxygenate but avoid using a bag-valve mask. If bagging is required, take a gentle and deliberate approach to avoid aspiration (approximately 10 breaths per minute).
- Intubate the patient with the head of bead elevated at 45 degrees. The best laryngoscope is the one you are most comfortable with. However, emesis can easily obscure the view of a video laryngoscope. Ensure you also have a direct laryngoscope available if you choose to use a video laryngoscope as your first line.
- For more, please see this post from EPMonthly.
Patients with active and massive UGIB need emergent endoscopy. For instances where patients might require stabilization prior to endoscopy or might require transfer to a higher level of care, consider balloon tamponade.19 This is a rare procedure performed as a “hail-Mary” attempt to save the patient. EMCrit has a detailed post on several different ways you can place a Blakemore tube or equivalent. EMRAP also has a video on tube placement and recent podcast of balloon tamponade. We briefly review the placement of a Blakemore device below.
Steps of Blakemore placement19
- The patient should be intubated as discussed above.
- Insert the tube via the esophagus to a depth of 50 cm
- Confirm the tube is in the stomach by aspirating gastric contents via gastric port
- Inflate the gastric balloon with 50 ml of air
- Confirm placement within the stomach using plain films
- Inflate the gastric balloon with 200 ml of additional air for total volume of 250 ml
- Put traction on the tube (using a pulley system with a liter bag of saline or equivalent weight)
- The traction and gastric balloon should be sufficient to tamponade most varies
- If bleeding continues, inflate the esophageal balloon
- Get a manometer! Do not inflate the esophageal balloon without a manometer
- Attach a manometer to the second 3-way stopcock on the esophageal port of the Blakemore. Inflate to 30 mm Hg. If bleeding continues, inflate to 45 mm Hg.
Endoscopic Therapy
Endoscopic therapy includes injection of epinephrine, bipolar electrocoagulation, band ligation, heater probe coagulation, laser photocoagulation, and ligation clips, such as Hemoclips.1,22 Numerous factors from the patient’s history, physical exam, and initial labs have been associated with the need for early endoscopic intervention. Specifically, the most predictive factors for endoscopic intervention are a history of malignancy or cirrhosis, presentation with fresh blood hematemesis, signs of hypovolemia including hypotension, tachycardia, shock, and a hemoglobin less than 8 g/dL at initial presentation.4,20
For non-variceal bleeding, the ACG recommends diagnostic and therapeutic endoscopy within 24 hours of admission.22However, recent studies have compared urgent endoscopy with elective endoscopy in hemodynamically stable patients and found no difference in clinical outcomes.20-21 In contrast, hemodynamically unstable patients with presumed UGIB should undergo endoscopy as early as possible after stabilization.10 Furthermore, patients with variceal bleeds require even sooner endoscopies, ideally within 12 hours.4,20,22 In cases of patients with ongoing variceal bleeding despite endoscopic intervention or when endoscopy cannot be performed emergently, a balloon tamponade should be considered as mentioned above.
Disposition
Several clinical tools and scoring systems have been developed and validated to help triage patients with acute upper GI bleed, identify those who need urgent endoscopic evaluation, and predict outcomes.2,22-25 These scoring systems include admission Rockall, full Rockall, Glasgow-Blatchford Score (GBS), AIMS65, and Progetto Nazionale Emorragia Digestiva (PNED). The Full Rockall and PNED scores require endoscopy for calculation and are not useful in the ED.12-25 Admission Rockall, GBS, and AIMS65 are pre-endoscopic scores which use clinical, hemodynamic, and laboratory values to help risk stratify patients.1,2 Studies have shown that these scores can be equally useful in identifying patients who might require urgent endoscopy, or management in high dependency, or those that can be treated in an outpatient setting.22-25
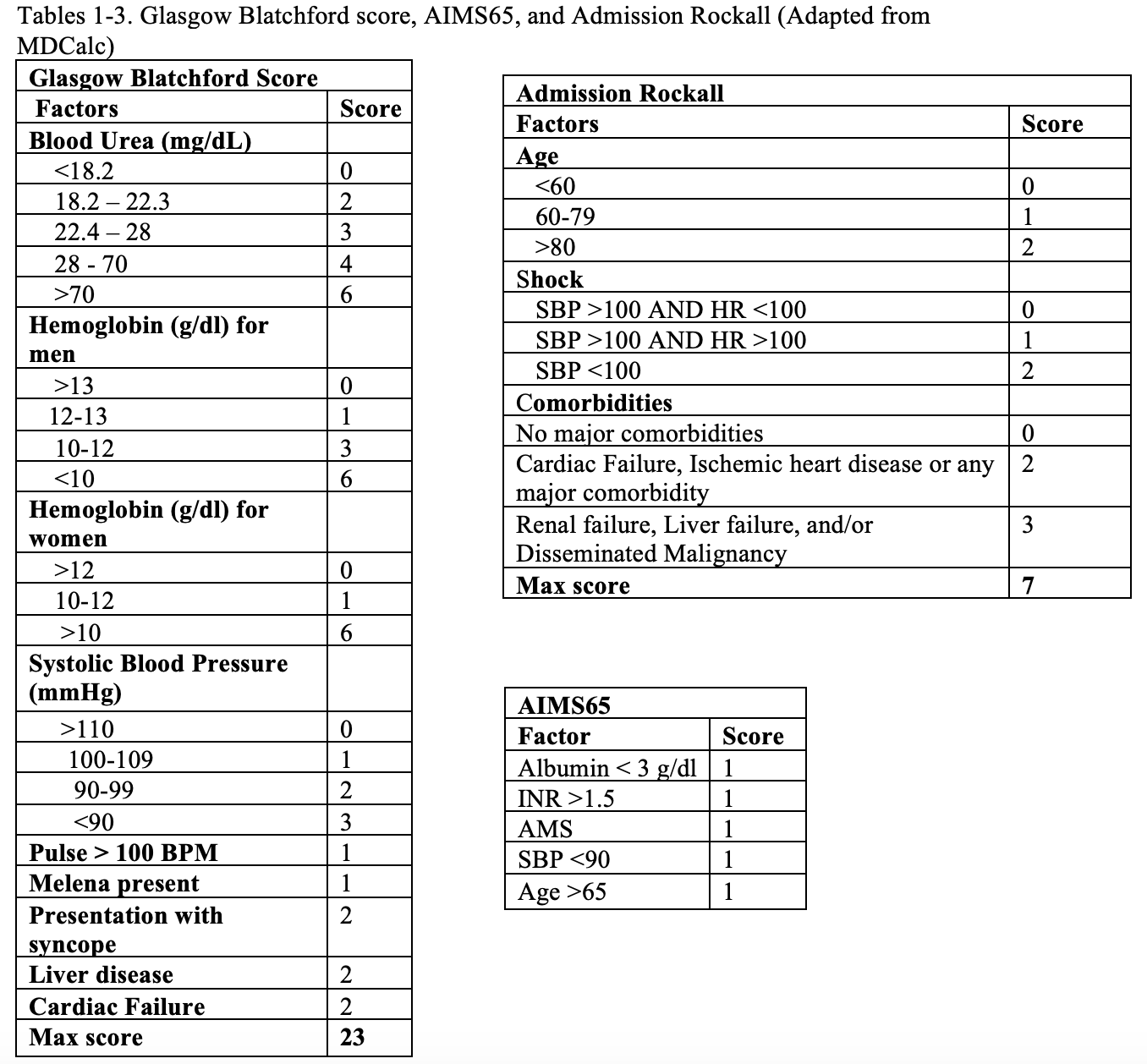
Stanley et al. performed a multicenter prospective study across six large hospitals in Europe, North American, Asia, and Oceania to compare the predicative accuracy and clinical utility of the five scoring systems.24 The study also found the optimal scoring threshold for identifying low- and high-risk patients. In this study the GBS had the highest discriminative ability at predicting need for intervention or death compared to the other four systems.24 A GBS of 1 or less had a sensitivity of 98.6% and specificity of 34.6% for predicting patients who were very low-risk and who did not require intervention.24 The GBS also performed better in predicting need for endoscopic treatment.24 A GBS of 7 or more was best at predicting the need for endoscopic treatment with sensitivity of 80.4% and specificity of 57.4%.24
Several studies have looked at expanding the threshold of GBS for discharge and safe outpatient management.25-27 Most studies have found that a GBS score of less than 2 is deemed low-risk, and the patient can be safely managed in an outpatient setting.25-27 Chatten et al investigated if the discharge threshold could be expanded to a GBS score of 2 to reduce the number of hospital days and help safely discharge these low-risk patients.25 The investigators retrospectively studied 399 patients hospitalized with symptoms of UGIB between October 2013 to June 2016 and found that the negative predictive value for excluding the need for endoscopic intervention with a GBS score of 1 was 100%, and extending to GBS of 2 reduces the negative predictive value to 98.53%.25 This study also found that only two patients with score of 2 required endoscopic therapy, both of which required variceal banding.25 The authors conclude that patients with non-variceal bleeds, and a GBS of 2 or less could be safely discharged with early outpatient management.25Current guidelines from the ACG state that patient with GBS score of 0 can be safely discharged from the ED. These patients have less than 1% chance of requiring intervention.12
AIMS65 and PNED score were similar at predicting 30-day mortality. AIMS65 was better at predicting mortality than GBS.23 The best score threshold for predicting 30-day mortality and the need for ICU admission was an AIMS65 score of 2 or greater.22-23
In the ED, we recommend using GBS to help risk stratify patients with UBIG. GBS scores of 0 can be safely discharged with close outpatient followup.12 For patients with a GBS of 1 or 2, use shared decision-making strategies with the patient and the GI specialist to determine admission vs discharge, with the caveat that patient does not have a score of 2 with liver disease.24-27 Patients with liver disease have high risk of varies and should be admitted.25 Depending on the overall clinical status, resources in the community, patients with a GBS of 1 could be discharged with next day follow up with GI specialists for outpatient endoscopy.25-27 It should be emphasized that while scoring system help risk stratify patients, no scoring system should not override clinical judgement or anticipated clinical course of a patient.
Case Conclusion
Case 1: The patient continued to remain hemodynamically stable in the ED. Lab work was remarkable for a Hgb of 12, BUN of 18, and INR of 1. Her GBS was 2. The patient was given a dose of IV pantoprazole in the ED. The provider spoke with the GI specialist and the patient was scheduled for next day follow-up with an elective endoscopy. The patient was prescribed PPI and told to stop taking NSAIDs. The patient felt comfortable with discharge with strict return precautions.
Case 2: The patient continued to have episodes of large volume hematemesis and started to become confused. The patient was transfused one unit of pRBCs and started on an IV PPI, along with Octreotide and Ceftriaxone. The patient was intubated, and an NG tube was placed that put out bright red blood. The ED physician consulted GI and the medical ICU for admission. The patient continued to receive blood products and underwent an emergent upper endoscopy for variceal band ligation.
Take Home Points
- Patients with UGIB can decompensate rapidly. Establish two large-bore IVs, and begin resuscitation as quickly as possible.
- Secure the airway early, and be prepared for a difficult airway.
- A through history and physical exam will help with the risk stratification of UGIB.
- Risk stratification scores can help identify who is low risk, intermediate risk and high risk.
- Patients with non-variceal bleeds who are low-risk can be discharged home with proper follow-up.
- Patients with variceal bleed carry a high mortality and need to be admitted for endoscopy.
References/Further Reading:
- Nelms DW, Pelaez CA. The Acute Upper Gastrointestinal Bleed. Surgical Clinics of North America. 2018;98(5):1047-1057. doi:10.1016/j.suc.2018.05.004
- Khamaysi I, Gralnek IM. Acute upper gastrointestinal bleeding (UGIB) – initial evaluation and management. Best Pract Res Clin Gastroenterol. 2013;27(5):633-638. doi:10.1016/j.bpg.2013.09.002
- Lanas A, Dumonceau JM, Hunt RH, et al. Non-variceal upper gastrointestinal bleeding. Nat Rev Dis Primers. 2018;4:18020. Published 2018 Apr 19. doi:10.1038/nrdp.2018.20
- Kamboj AK, Hoversten P, Leggett CL. Upper Gastrointestinal Bleeding: Etiologies and Management. Mayo Clin Proc. 2019;94(4):697-703. doi:10.1016/j.mayocp.2019.01.022
- Lee E, Kim YJ, Goo DE, et al. Comparison of hepatic venous pressure gradient and endoscopic grading of esophageal varices. World J Gastroenterol. 2016;22(11):3212-3219. doi:10.3748/wjg.v22.i11.3212
- Friedman A, Chan A, Chin LC, et al. Use and abuse of faecal occult blood tests in an acute hospital inpatient setting. Intern Med J. 2010;40(2):107-111. doi:10.1111/j.1445-5994.2009.02149.x
- Sharma VK, Komanduri S, Nayyar S, et al. An audit of the utility of in-patient fecal occult blood testing. Am J Gastroenterol. 2001;96(4):1256-1260. doi:10.1111/j.1572-0241.2001.03709.x
- Patrick Radecki, R., 2021. It’s Time to Abandon Fecal Occult Blood Testing in the Emergency Department. ACEP Now. Available at: <https://www.acepnow.com/article/its-time-to-abandon-fecal-occult-blood-testing-in-the-emergency-department/>
- Ernst AA, Haynes ML, Nick TG, Weiss SJ. Usefulness of the blood urea nitrogen/creatinine ratio in gastrointestinal bleeding. Am J Emerg Med. 1999;17(1):70-72. doi:10.1016/s0735-6757(99)90021-9
- Al Duhailib Z, Dionne JC, Alhazzani W. Management of severe upper gastrointestinal bleeding in the ICU. Curr Opin Crit Care. 2020;26(2):212-218. doi:10.1097/MCC.0000000000000699
- Lau JYW. Evidence-based management of patients with acute non-variceal upper gastrointestinal bleeding. Gastrointestinal Intervention. 2012;1(1):53-57. doi:10.1016/j.gii.2012.09.002
- Laine L, Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107(3):345-361. doi:10.1038/ajg.2011.480
- Sachar H, Vaidya K, Laine L. Intermittent vs continuous proton pump inhibitor therapy for high-risk bleeding ulcers: a systematic review and meta-analysis. JAMA Intern Med. 2014;174(11):1755-1762. doi:10.1001/jamainternmed.2014.4056
- Bañares R, Albillos A, Rincón D, et al. Endoscopic treatment versus endoscopic plus pharmacologic treatment for acute variceal bleeding: a meta-analysis. Hepatology. 2002;35(3):609-615. doi:10.1053/jhep.2002.31354
- Lee YY, Tee HP, Mahadeva S. Role of prophylactic antibiotics in cirrhotic patients with variceal bleeding. World J Gastroenterol. 2014;20(7):1790-1796. doi:10.3748/wjg.v20.i7.1790
- Nickson C. Intubation in Upper Gastrointestinal Haemorrhage • LITFL • CCC Airway. Life in the Fast Lane. https://litfl.com/intubation-in-upper-gastrointestinal-haemorrhage/. Published 2021. Accessed May 5, 2021.
- Weingart S. Intubating the Critical GI Bleeder. org. https://emcrit.org/emcrit/intubating-gi-bleeds/. Published 2009. Accessed May 5, 2021.
- Ducanto J, Serrano KD, Thompson RJ. Novel Airway Training Tool that Simulates Vomiting: Suction-Assisted Laryngoscopy Assisted Decontamination (SALAD) System. West J Emerg Med. 2017;18(1):117-120.
- Weingart S. Blakemore Tube Placement for Massive Upper GI Hemorrhage. Emcrit.org. https://emcrit.org/emcrit/blakemore-tube-placement/. Published 2013. Accessed May 5, 2021.
- Srygley FD, Gerardo CJ, Tran T, Fisher DA. Does this patient have a severe upper gastrointestinal bleed? JAMA. 2012;307(10):1072-1079. doi:10.1001/jama.2012.253
- Bjorkman DJ, Zaman A, Fennerty MB, et al. Urgent vs. elective endoscopy for acute nonvariceal upper-GI bleeding: an effectiveness study. Gastrointest Endosc 2004; 60:1–8
- Chen IC, Hung MS, Chiu TF, Chen JC, Hsiao CT. Risk scoring systems to predict need for clinical intervention for patients with nonvariceal upper gastrointestinal tract bleeding. Am J Emerg Med. 2007;25(7):774-779. doi:10.1016/j.ajem.2006.12.024
- Robertson M, Majumdar A, Boyapati R, et al. Risk stratification in acute upper GI bleeding: comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems. Gastrointest Endosc. 2016;83(6):1151-1160. doi:10.1016/j.gie.2015.10.021
- Stanley AJ, Laine L. Management of acute upper gastrointestinal bleeding. BMJ. 2019;364:l536. Published 2019 Mar 25. doi:10.1136/bmj.l536
- Chatten K, Purssell H, Banerjee AK, Soteriadou S, Ang Y. Glasgow Blatchford Score and risk stratifications in acute upper gastrointestinal bleed: can we extend this to 2 for urgent outpatient management? Clin Med (Lond). 2018;18(2):118-122. doi:10.7861/clinmedicine.18-2-118
- Masaoka T, Suzuki H, Hori S, Aikawa N, Hibi T. Blatchford scoring system is a useful scoring system for detecting patients with upper gastrointestinal bleeding who do not need endoscopic intervention. J Gastroenterol Hepatol. 2007;22(9):1404-1408. doi:10.1111/j.1440-1746.2006.04762.x
- Srirajaskanthan R, Conn R, Bulwer C, Irving P. The Glasgow Blatchford scoring system enables accurate risk stratification of patients with upper gastrointestinal haemorrhage. Int J Clin Pract. 2010;64(7):868-874. doi:10.1111/j.1742-1241.2009.02267.x






